 Long covid, omicron and the precautionary principle
Long covid, omicron and the precautionary principle
Written By:
- Date published:
1:12 pm, December 20th, 2021 - 95 comments
Categories: covid-19, disability, long covid -
Tags: M.E., omicron, precautionary principle
I’m relieved to see New Zealand starting to look at long covid. Our relatively low covid infection rate has meant this hasn’t been prominent in the pandemic response debate. The arrival of the very fast spreading omicron variant points to now being the time to look at the long range covid forecast, not just how to get back to normal.
I’ve been following people with long covid online, including in NZ, since near the start of the pandemic, and it’s been obvious from early on that this is a serious condition for individuals and for society. Long covid is when people either don’t fully recover from covid, or they recover and then get related symptoms some time later. Some of these symptoms are sustained for a while and then leave, some just seem to stay. Some are less problematic, some are very serious, and some create long term disability. It can affect nearly any organ system in the body, making it a complex syndrome rather than a discrete, easily understandable illness.
Estimates of how many people with covid end up with long term symptoms vary. I’ve heard the MoH is using a 10% rate but internationally it’s more like up to 40%. It also depends on how long covid is defined. I’m not referencing much, because I think this is such a new area and there are going to be a lot of competing ideas and data sources out there. In other words, we just don’t know yet how this will work with omicron. I’m less interested in arguing selective data than I am in looking at the importance of caution, and why the precautionary principle is sound.
Mainstream media in New Zealand have been reporting on a recent study on pre-omicron long covid. RNZ in October,
According to a new study from Oxford University, 37 percent of infected had at least one long Covid symptom diagnosed.
“Two hundred and seventy thousand Covid survivors, and they followed them, and between a third and a half had symptoms three to six months later,” Potter said speaking today to Saturday Morning.
“And those are a wide variety of symptoms that are indicative of the fact that this particular virus infects a lot of different parts of us. It’s not just a respiratory virus.”
“It’s a virus that gets into lots of organs and has downstream consequences that are really nasty for a lot of people.”
Long Covid symptoms can include breathing problems, abdominal symptoms, fatigue, pain, anxiety and depression.
Victims can have myalgia, pain in the muscles, which can present similar to chronic fatigue syndrome.
“Abnormal breathing persists in a decent percentage of people almost 20 percent of people because of damage to the lungs,” Potter said.
“Some people have headaches and cognitive symptoms which tells us that it does damage to the brain.”
From the CDC’s clinical care page on long covid,
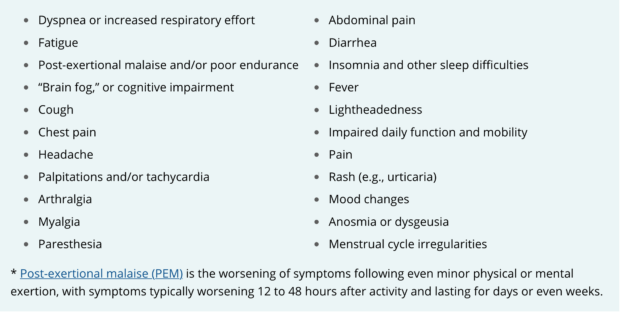
It’s worth pointing out here that this is a novel illness. Which means that we don’t actually know what we are dealing with yet. In part because we haven’t had enough time to see how this plays out over time. And because it takes time to do medical research.
It’s also worth pointing out the similarities with Myalgic Encephalomyelitis, a chronic illness that the medical profession has long struggled to even understand let alone treat. M.E. is also quaintly known as Chronic Fatigue Syndrome, which is akin to calling tuberculosis Chronic Cough Syndrome. Minimisation is part of a pattern that plays into priorities in medical funding, and governmental responses in the Health and Welfare systems, as well as prejudices in society.
Of particular note in that chart is the presence of Post-Exertional Malaise, one of the key indicators of M.E. and a symptom that means normal activity can become very constrained as it worsens fatigue and other symptoms. M.E. is also known as post-viral syndrome, and there is now research looking at the similarities between the two illnesses.
I’m not sure if we know much yet about how long covid plays out in vaccinated and unvaccinated people, but obviously unvaccinated people are more likely to get covid in the first place, so have an increased risk of long covid. This from Australian data geeks on pre-omicron long covid in NZ,
Long COVID has the potential to really disrupt businesses beyond just a few weeks of infection.
We project that 2.7% of all unvaxxed employees will be working reduced hours 7 months after a COVID infection, and another 1.3% won't be working at all.— Emma Vitz (@EmmaVitz) December 16, 2021
We also don’t know a lot yet about how long covid will impact on people with already existing other health disabilities. And for those thinking that they’re sweet because they have no pre-existing conditions so covid is unlikely to affect them much, M.E. hits some very fit and healthy people hard, and it’s unclear how those without comorbidities are affected.
There are additional issues for children, and groups of people already at a higher risk from covid eg Māori and people living in poverty.
So what are the concerns here? Foremost is that people who contract covid are also then at risk of long term disability. Not just some annoying symptoms that drag on, but life altering disability.
I really think most people's conception of Long Covid is "I'll get a little winded walking up stairs" and not "I'll get an incurable neurological disease worthy of an Oliver Sacks book" and that's a communication problem
— Baby Ruthless
(@babyrelentless) December 17, 2021
That obviously is also a big issue for the State. What will be the impact on the Health and Welfare budgets? Will productivity be affected? Will front line workers, including in highly trained professions like nurses and doctors, be disproportionately affected and how will this impact on the wider health system? I don’t think I’ve seen the government talk about this.
There’s also the grim and bleak prospect that people who become unable to work from long covid will have their lives changed in other ways. Work and Income current payment rates:
- $278 in the hand per week to single people with no children, on the dole with a medical exemption (what replaced the Sickness Benefit).
- Supported Living Payment, for long term illness and disability, is $336. It’s hard to get onto SLP, many long term disabled people are living on the dole
- Disability Allowance is capped at $66/wk.
- Accommodation Supplement varies depending on where you live and what your accommodation costs are. If you have cash assets (savings but also any large asset that isn’t your home), you won’t be eligible. Any more than $8,100 for a single person and you will be expected to use that before you get can get AS.
- Temporary Additional Support also varies, and is capped at 30% of your applied for costs. It’s meant to be a stop gap, but is the benefit many long termers rely on to survive. It requires a fair amount of hoop jumping to get and retain. It is also asset and income tested.
I’m laying this out because I want it to be clear that Labour and New Zealand generally are ok with that situation. In the long years that Labour has been dragging on sorting welfare rates, there’s been almost nothing from them about the rates of people who cannot work due to disability.
It’s also in the health system, where people with chronic illnesses, sometimes severely disabling, often get very little in the way of practical assistance at home.
We know that people on benefits because of disability and illness also face particular discrimination. Then Labour leader David Shearer’s 2012, dog whistling, painter-on-the-roof speech to Grey Power was both shocking and unsurprising as Shearer empathised with the good working class man who goes out to earn for the family everyday while his bad neighbour on sickness benefit is up painting his roof. Long covid already includes invisible disability. You can’t see PEM, pain levels, or any number of the other symptoms, and prejudice is built into our governance systems.
The benefit bludger memes get applied on steroids to ill people who don’t look disabled enough, who are not just bludgers but malingerers.
All of that is the result of long standing state discrimination against disabled people, those with chronic illnesses in particular.
There is some hope here that long covid will wake up the government and medical profession, and we will see a change in attitude. But let’s not forget that when the pandemic first arrived, we were going into lockdown, and Labour were giving out money to businesses and workers, people on benefits had to wait for any financial assistance. Which meant no extra cash to buy masks, hand sanitiser, or bulk food so they could avoid crowded places. This is a long standing attitude towards disabled beneficiaries in particular. Get to the back of the queue.
This at RNZ from Jenene Crossan, 37th person in NZ to test positive for covid (in 2020) and covid long hauler, speaks to the attitudes to long covid,
Sufferers “can’t get ACC, they’re not getting any kind of public health response, they’re being ignored in the public health system, they’re being pushed back saying ‘we have no place for you, we don’t know what to do with you’, being gaslit. “We don’t believe in Long Covid’ – they’re hearing that from GPs still.
“There’s no pathway, there’s no protocols, there’s no official information about whether we should be getting the vaccines or not. There’s a lot of ‘yes we plan on… ‘ but not a lot of ‘yes we’re doing’.”
So those say Omicron is ‘mild’. Just be mindful. This is what a mild case looks like. #TreatLongCovid
— Dr K Fearnley (@fearnley_k) December 18, 2021
For people struggling with the restrictions of the pandemic response, there is a not much talked about dynamic of the relationship between constraint and freedom. If long covid affects between 10% and 40% of people that contract covid, what should we then make of the arguments for open borders, no more lock downs, and letting it rip until we have natural or herd immunity? What if natural immunity is something that we can gain in later years, once covid has settled into a more recognisable pattern but is premature now? If we increase community transmission, what are the likelihoods of further variants that may or may not be more deadly and may or may not be associated with higher levels of long covid?
We just don’t know.
New Zealand is still in a fairly unique position in the world because of our low community transmission rates. Omicron presents new challenges. The precautionary principle tells us that we can act to prevent disability as well as death, and that we can keep our future options open by being careful now. The alternative is that we gamble future freedoms for short term gain.
To me long covid looks like a shit show waiting to happen on multiple, life destroying levels. We should be taking it extremely seriously, and learning from the experiences of people with similar chronic illnesses.
95 comments on “Long covid, omicron and the precautionary principle ”
- Comments are now closed
- Comments are now closed
Recent Comments
- Northern Australia: fortress, gateway and resource powerhouse
 In the week of Australia’s 3 May election, ASPI will release Agenda for Change 2025: preparedness and resilience in an uncertain world, a report promoting public debate and understanding on issues of strategic importance to ...4 hours ago
In the week of Australia’s 3 May election, ASPI will release Agenda for Change 2025: preparedness and resilience in an uncertain world, a report promoting public debate and understanding on issues of strategic importance to ...4 hours ago - Bernard’s Saturday Soliloquy for the week to April 26
 Chris Bishop has unveiled plans for new roads in Tauranga, Auckland and Northland that will cost up to a combined $10 billion. Photo: Lynn GrievesonLong stories short from Aotearoa political economy around housing, poverty and climate in the week to Saturday, April 26:Chris Bishop ploughed ahead this week with spending ...6 hours ago
Chris Bishop has unveiled plans for new roads in Tauranga, Auckland and Northland that will cost up to a combined $10 billion. Photo: Lynn GrievesonLong stories short from Aotearoa political economy around housing, poverty and climate in the week to Saturday, April 26:Chris Bishop ploughed ahead this week with spending ...6 hours ago - Debt Is A Form Of Government Control
 Unless you've been living under a rock, you would have noticed that New Zealand’s government, under the guise of economic stewardship, is tightening the screws on its citizens, and using debt as a tool of control. This isn’t just a conspiracy theory whispered in pub corners...it’s backed by hard data ...8 hours ago
Unless you've been living under a rock, you would have noticed that New Zealand’s government, under the guise of economic stewardship, is tightening the screws on its citizens, and using debt as a tool of control. This isn’t just a conspiracy theory whispered in pub corners...it’s backed by hard data ...8 hours ago - The 2025 Budget in a World of Trade Warfare
 The budget runup is far from easy.Budget 2025 day is Thursday 22 May. About a month earlier in a normal year, the macroeconomic forecasts would be completed (the fiscal ones would still be tidying up) and the main policy decisions would have been made (but there would still be a ...20 hours ago
The budget runup is far from easy.Budget 2025 day is Thursday 22 May. About a month earlier in a normal year, the macroeconomic forecasts would be completed (the fiscal ones would still be tidying up) and the main policy decisions would have been made (but there would still be a ...20 hours ago - EGU2025 – Presentation about our translation activities
 As mentioned in the recently published prolog to EGU2025 article, I submitted an abstract to talk about some of our translation activities and the challenges we have been facing with those. This blog post is a "companion article" to that presentation in session EOS4.3 Geoethics and Global Anthropogenic Change: Geoscience for Policy, ...21 hours ago
As mentioned in the recently published prolog to EGU2025 article, I submitted an abstract to talk about some of our translation activities and the challenges we have been facing with those. This blog post is a "companion article" to that presentation in session EOS4.3 Geoethics and Global Anthropogenic Change: Geoscience for Policy, ...21 hours ago - The drums of war revisited
On 25 April 2021, I published an internal all-staff Anzac Day message. I did so as the Secretary of the Department of Home Affairs, which is responsible for Australia’s civil defence, and its resilience in ...1 day ago
- Cameron Slater’s New Website: Same Old Defamation
You’ve likely noticed that the disgraced blogger of Whale Oil Beef Hooked infamy, Cameron Slater, is still slithering around the internet, peddling his bile on a shiny new blogsite calling itself The Good Oil. If you thought bankruptcy, defamation rulings, and a near-fatal health scare would teach this idiot a ...1 day ago
- David Seymour’s Atlas Network Receiving Unwanted Attention
The Atlas Network, a sprawling web of libertarian think tanks funded by fossil fuel barons and corporate elites, has sunk its claws into New Zealand’s political landscape. At the forefront of this insidious influence is David Seymour, the ACT Party leader, whose ties to Atlas run deep.With the National Party’s ...1 day ago
- Nicola Willis To Blame For Family Boost Debacle
Nicola Willis, National’s supposed Finance Minister, has delivered another policy failure with the Family Boost scheme, a childcare rebate that was big on promises but has been very small on delivery. Only 56,000 families have signed up, a far cry from the 130,000 Willis personally championed in National’s campaign. This ...1 day ago
- Editors’ pick: ‘On the value of military service’
This article was first published on 7 February 2025. In January, I crossed the milestone of 24 years of service in two militaries—the British and Australian armies. It is fair to say that I am ...1 day ago
- Rest easy, my friend.
 He shall grow not old, as we that are left grow old.Age shall not weary him, nor the years condemn.At the going down of the sun and in the morningI will remember him.My mate Keith died yesterday, peacefully in the early hours. My dear friend in Rotorua, whom I’ve been ...1 day ago
He shall grow not old, as we that are left grow old.Age shall not weary him, nor the years condemn.At the going down of the sun and in the morningI will remember him.My mate Keith died yesterday, peacefully in the early hours. My dear friend in Rotorua, whom I’ve been ...1 day ago - The Hoon around the week to April 25
 The podcast above of the weekly ‘Hoon’ webinar for paying subscribers on Thursday night features co-hosts & talking about the week’s news with regular and special guests, including: on news New Zealand abstained from a vote on a global shipping levy on climate emissions and downgraded the importance ...1 day ago
The podcast above of the weekly ‘Hoon’ webinar for paying subscribers on Thursday night features co-hosts & talking about the week’s news with regular and special guests, including: on news New Zealand abstained from a vote on a global shipping levy on climate emissions and downgraded the importance ...1 day ago - The Men Commenting on Lorde
 Hi,In case you missed it, New Zealand icon Lorde has a new single out. It’s called “What Was That”, and has a very low key music video that was filmed around her impromptu performance in New York’s Washington Square Park. When police shut down the initial popup, one of my ...1 day ago
Hi,In case you missed it, New Zealand icon Lorde has a new single out. It’s called “What Was That”, and has a very low key music video that was filmed around her impromptu performance in New York’s Washington Square Park. When police shut down the initial popup, one of my ...1 day ago - Skeptical Science New Research for Week #17 2025
Open access notables Internal variability effect doped by climate change drove the 2023 marine heat extreme in the North Atlantic, Guinaldo et al., Communications Earth & Environment The year 2023 shattered numerous heat records both globally and regionally. We here focus on the drivers of the unprecedented warm sea surface temperature (SST) anomalies which started in ...2 days ago
- Military denial: the basis of deterrence, and of response if deterrence fails
A strategy of denial is now the cornerstone concept for Australia’s National Defence Strategy. The term’s use as an overarching guide to defence policy, however, has led to some confusion on what it actually means ...2 days ago
- Fiscal failure
 The IMF’s twice-yearly World Economic Outlook and Fiscal Monitor publications have come out in the last couple of days. If there is gloom in the GDP numbers (eg this chart for the advanced countries, and we don’t score a lot better on the comparable one for the 2019 to ...2 days ago
The IMF’s twice-yearly World Economic Outlook and Fiscal Monitor publications have come out in the last couple of days. If there is gloom in the GDP numbers (eg this chart for the advanced countries, and we don’t score a lot better on the comparable one for the 2019 to ...2 days ago - Climate Change: Fucking the ETS again
 For a while, it looked like the government had unfucked the ETS, at least insofar as unit settings were concerned. They had to be forced into it by a court case, but at least it got done, and when National came to power, it learned the lesson (and then fucked ...2 days ago
For a while, it looked like the government had unfucked the ETS, at least insofar as unit settings were concerned. They had to be forced into it by a court case, but at least it got done, and when National came to power, it learned the lesson (and then fucked ...2 days ago - What’s secret? When is it secret? Well, that’s complicated
The argument over US officials’ misuse of secure but non-governmental messaging platform Signal falls into two camps. Either it is a gross error that undermines national security, or it is a bit of a blunder ...2 days ago
- Today’s Headlines: David Seymour’s ECE Risks & Coalition Government Lies
 Cost of living ~1/3 of Kiwis needed help with food as cost of living pressures continue to increase - turning to friends, family, food banks or Work and Income in the past year, to find food. 40% of Kiwis also said they felt schemes offered little or no benefit, according ...2 days ago
Cost of living ~1/3 of Kiwis needed help with food as cost of living pressures continue to increase - turning to friends, family, food banks or Work and Income in the past year, to find food. 40% of Kiwis also said they felt schemes offered little or no benefit, according ...2 days ago - Is The NZ Media Awards Sponsored By a Conspiracy Theorist?
 Hi,Perhaps in 2025 it shouldn’t come as a surprise that the CEO and owner of Voyager Internet — the major sponsor of the New Zealand Media Awards — has taken to sharing a variety of Anti-Muslim and anti-Jewish conspiracy theories to his 1.2 million followers.This included sharing a post from ...2 days ago
Hi,Perhaps in 2025 it shouldn’t come as a surprise that the CEO and owner of Voyager Internet — the major sponsor of the New Zealand Media Awards — has taken to sharing a variety of Anti-Muslim and anti-Jewish conspiracy theories to his 1.2 million followers.This included sharing a post from ...2 days ago - Australia-India defence cooperation should be about more than navies
In the sprint to deepen Australia-India defence cooperation, navy links have shot ahead of ties between the two countries’ air forces and armies. That’s largely a good thing: maritime security is at the heart of ...2 days ago
- When in Rome
 'Cause you and me, were meant to be,Walking free, in harmony,One fine day, we'll fly away,Don't you know that Rome wasn't built in a day?Songwriters: Paul David Godfrey / Ross Godfrey / Skye Edwards.I was half expecting to see photos this morning of National Party supporters with wads of cotton ...2 days ago
'Cause you and me, were meant to be,Walking free, in harmony,One fine day, we'll fly away,Don't you know that Rome wasn't built in a day?Songwriters: Paul David Godfrey / Ross Godfrey / Skye Edwards.I was half expecting to see photos this morning of National Party supporters with wads of cotton ...2 days ago - Thursday 24 April
 The PSA says a settlement with Health New Zealand over the agency’s proposed restructure of its Data and Digital and Pacific Health teams has saved around 200 roles from being cut. A third of New Zealanders have needed help accessing food in the past year, according to Consumer NZ, and ...2 days ago
The PSA says a settlement with Health New Zealand over the agency’s proposed restructure of its Data and Digital and Pacific Health teams has saved around 200 roles from being cut. A third of New Zealanders have needed help accessing food in the past year, according to Consumer NZ, and ...2 days ago - John Campbell Investigates Brian Tamaki’s Destiny Church
John Campbell’s Under His Command, a five-part TVNZ+ investigation series starting today, rips the veil off Destiny Church, exposing the rot festering under Brian Tamaki’s self-proclaimed apostolic throne. This isn’t just a church; it’s a fiefdom, built on fear, manipulation, and a trail of scandals that make your stomach churn. ...2 days ago
- Decrypting tomorrow’s threats: critical infrastructure needs post-quantum protection today
Some argue we still have time, since quantum computing capable of breaking today’s encryption is a decade or more away. But breakthrough capabilities, especially in domains tied to strategic advantage, rarely follow predictable timelines. Just ...2 days ago
- Inside my quest for a climate-friendly bank
This is a re-post from Yale Climate Connections by Pearl Marvell (Photo credit: Pearl Marvell. Image credit: Samantha Harrington. Dollar bill vector image: by pch.vector on Freepik) Igrew up knowing that when you had extra money, you put it under a bed, stashed it in a book or a clock, or, ...2 days ago
- Winston Peters Has Lost The Plot
The political petrified piece of wood, Winston Peters, who refuses to retire gracefully, has had an eventful couple of weeks peddling transphobia, pushing bigoted policies, undertaking his unrelenting war on wokeness and slinging vile accusations like calling Green co-leader Chlöe Swarbrick a “groomer”.At 80, the hypocritical NZ First leader’s latest ...2 days ago
- The one who left
 It's raining in Cockermouth and we're following our host up the stairs. We’re telling her it’s a lovely building and she’s explaining that it used to be a pub and a nightclub and a backpackers, but no more.There were floods in 2009 and 2015 along the main street, huge floods, ...2 days ago
It's raining in Cockermouth and we're following our host up the stairs. We’re telling her it’s a lovely building and she’s explaining that it used to be a pub and a nightclub and a backpackers, but no more.There were floods in 2009 and 2015 along the main street, huge floods, ...2 days ago - Gordon Campbell On The Trump Upside, And Peters Persecution Of Trans People
 A recurring aspect of the Trump tariff coverage is that it normalises – or even sanctifies – a status quo that in many respects has been a disaster for working class families. No doubt, Donald Trump is an uncertainty machine that is tanking the stock market and the growth prospects ...3 days ago
A recurring aspect of the Trump tariff coverage is that it normalises – or even sanctifies – a status quo that in many respects has been a disaster for working class families. No doubt, Donald Trump is an uncertainty machine that is tanking the stock market and the growth prospects ...3 days ago - Is Mark Mitchell a racist?
The National Party’s Minister of Police, Corrections, and Ethnic Communities (irony alert) has stumbled into yet another racist quagmire, proving that when it comes to bigotry, the right wing’s playbook is as predictable as it is vile. This time, Mitchell’s office reposted an Instagram reel falsely claiming that Te Pāti ...3 days ago
- Australian statecraft must restore the link between deterrence and non-proliferation to survive in t...
In the week of Australia’s 3 May election, ASPI will release Agenda for Change 2025: preparedness and resilience in an uncertain world, a report promoting public debate and understanding on issues of strategic importance to ...3 days ago
- J.K. Rowling – Arsehole of the Week
In a world crying out for empathy, J.K. Rowling has once again proven she’s more interested in stoking division than building bridges. The once-beloved author of Harry Potter has cemented her place as this week’s Arsehole of the Week, a title earned through her relentless, tone-deaf crusade against transgender rights. ...3 days ago
- The rotten, unaccountable crown
Between 1950 and 1993 the New Zealand government tortured and abused up to 250,000 children in residential care facilities. They then proceeded to cover it up in order to minimise their liability, dragging out cases, slandering their victims and ultimately denying redress. In its final report, the Inquiry into Abuse ...3 days ago
- To prepare for future threats, treat health security as national security
Health security is often seen as a peripheral security domain, and as a problem that is difficult to address. These perceptions weaken our capacity to respond to borderless threats. With the wind back of Covid-19 ...3 days ago
- What’s on the Label -vs- What’s in the Tin.
 Would our political parties pass muster under the Fair Trading Act?WHAT IF OUR POLITICAL PARTIES were subject to the Fair Trading Act? What if they, like the nation’s businesses, were prohibited from misleading their consumers – i.e. the voters – about the nature, characteristics, suitability, or quantity of the products ...3 days ago
Would our political parties pass muster under the Fair Trading Act?WHAT IF OUR POLITICAL PARTIES were subject to the Fair Trading Act? What if they, like the nation’s businesses, were prohibited from misleading their consumers – i.e. the voters – about the nature, characteristics, suitability, or quantity of the products ...3 days ago - Simeon Brown Doesn’t Consider Abortion To Be Healthcare As Services Scaled Back
 Rod EmmersonThank you to my subscribers and readers - you make it all possible. Tui.Subscribe nowSix updates today from around the world and locally here in Aoteaora New Zealand -1. RFK Jnr’s Autism CrusadeAmerica plans to create a registry of people with autism in the United States. RFK Jr’s department ...3 days ago
Rod EmmersonThank you to my subscribers and readers - you make it all possible. Tui.Subscribe nowSix updates today from around the world and locally here in Aoteaora New Zealand -1. RFK Jnr’s Autism CrusadeAmerica plans to create a registry of people with autism in the United States. RFK Jr’s department ...3 days ago - Another Munich crisis? Understanding the limits of policymaking by analogy
We see it often enough. A democracy deals with an authoritarian state, and those who oppose concessions cite the lesson of Munich 1938: make none to dictators; take a firm stand. And so we hear ...3 days ago
- Wednesday 23 April
370 perioperative nurses working at Auckland City Hospital, Starship Hospital and Greenlane Clinical Centre will strike for two hours on 1 May – the same day senior doctors are striking. This is part of nationwide events to mark May Day on 1 May, including rallies outside public hospitals, organised by ...3 days ago
- Auckland character rules stop building on 20,000 sections
 Character protections for Auckland’s villas have stymied past development. Now moves afoot to strip character protection from a bunch of inner-city villas. Photo: Lynn Grieveson / The KākāLong stories shortest from our political economy on Wednesday, April 23:Special Character Areas designed to protect villas are stopping 20,000 sites near Auckland’s ...3 days ago
Character protections for Auckland’s villas have stymied past development. Now moves afoot to strip character protection from a bunch of inner-city villas. Photo: Lynn Grieveson / The KākāLong stories shortest from our political economy on Wednesday, April 23:Special Character Areas designed to protect villas are stopping 20,000 sites near Auckland’s ...3 days ago - AI is changing Indo-Pacific naval operations
Artificial intelligence is poised to significantly transform the Indo-Pacific maritime security landscape. It offers unprecedented situational awareness, decision-making speed and operational flexibility. But without clear rules, shared norms and mechanisms for risk reduction, AI could ...3 days ago
- What is a Man?
 For what is a man, what has he got?If not himself, then he has naughtTo say the things he truly feelsAnd not the words of one who kneelsThe record showsI took the blowsAnd did it my wayLyrics: Paul Anka.Morena folks, before we discuss Winston’s latest salvo in NZ First’s War ...3 days ago
For what is a man, what has he got?If not himself, then he has naughtTo say the things he truly feelsAnd not the words of one who kneelsThe record showsI took the blowsAnd did it my wayLyrics: Paul Anka.Morena folks, before we discuss Winston’s latest salvo in NZ First’s War ...3 days ago - Britain recasts AUKUS for a new era
Britain once risked a reputation as the weak link in the trilateral AUKUS partnership. But now the appointment of an empowered senior official to drive the project forward and a new burst of British parliamentary ...4 days ago
- Australia’s basic-metals problem: old plants and subsidised Chinese competition
Australia’s ability to produce basic metals, including copper, lead, zinc, nickel and construction steel, is in jeopardy, with ageing plants struggling against Chinese competition. The multinational commodities company Trafigura has put its Australian operations under ...4 days ago
- Rob Campbell – Public Private Partnerships: What a Good Idea! OR ‘There will be no free...
 There have been recent PPP debacles, both in New Zealand (think Transmission Gully) and globally, with numerous examples across both Australia and Britain of failed projects and extensive litigation by government agencies seeking redress for the failures.Rob Campbell is one of New Zealand’s sharpest critics of PPPs noting that; "There ...4 days ago
There have been recent PPP debacles, both in New Zealand (think Transmission Gully) and globally, with numerous examples across both Australia and Britain of failed projects and extensive litigation by government agencies seeking redress for the failures.Rob Campbell is one of New Zealand’s sharpest critics of PPPs noting that; "There ...4 days ago - RB spending: the Board and the Minister
On Twitter on Saturday I indicated that there had been a mistake in my post from last Thursday in which I attempted to step through the Reserve Bank Funding Agreement issues. Making mistakes (there are two) is annoying and I don’t fully understand how I did it (probably too much ...4 days ago
- Indonesia needs to rethink its approach to military drones
Indonesia’s armed forces still have a lot of work to do in making proper use of drones. Two major challenges are pilot training and achieving interoperability between the services. Another is overcoming a predilection for ...4 days ago
- Help Stop the Gaza Genocide Through Activism
As a living breathing human being, you’ve likely seen the heart-wrenching images from Gaza...homes reduced to rubble, children burnt to cinders, families displaced, and a death toll that’s beyond comprehension. What is going on in Gaza is most definitely a genocide, the suffering is real, and it’s easy to feel ...4 days ago
- Willis ignores new Global Financial & Trade Crisis
 Donald Trump, who has called the Chair of the Federal Reserve “a major loser”. Photo: Getty ImagesLong stories shortest from our political economy on Tuesday, April 22:US markets slump after Donald Trump threatens the Fed’s independence. China warns its trading partners not to side with the US. Trump says some ...4 days ago
Donald Trump, who has called the Chair of the Federal Reserve “a major loser”. Photo: Getty ImagesLong stories shortest from our political economy on Tuesday, April 22:US markets slump after Donald Trump threatens the Fed’s independence. China warns its trading partners not to side with the US. Trump says some ...4 days ago - One of the Good Ones
 4 days ago
4 days ago - AI is reshaping security, and the intelligence review sets good direction
The 2024 Independent Intelligence Review found the NIC to be highly capable and performing well. So, it is not a surprise that most of the 67 recommendations are incremental adjustments and small but nevertheless important ...4 days ago
- A worse-than-current-policy world?
This is a re-post from The Climate Brink The world has made real progress toward tacking climate change in recent years, with spending on clean energy technologies skyrocketing from hundreds of billions to trillions of dollars globally over the past decade, and global CO2 emissions plateauing. This has contributed to a reassessment of ...4 days ago
- “An A-Grade Teacher’s Pet”
 Hi,I’ve been having a peaceful month of what I’d call “existential dread”, even more aware than usual that — at some point — this all ends.It was very specifically triggered by watching Pantheon, an animated sci-fi show that I’m filing away with all-time greats like Six Feet Under, Watchmen and ...4 days ago
Hi,I’ve been having a peaceful month of what I’d call “existential dread”, even more aware than usual that — at some point — this all ends.It was very specifically triggered by watching Pantheon, an animated sci-fi show that I’m filing away with all-time greats like Six Feet Under, Watchmen and ...4 days ago - Gordon Campbell On Papal Picks, And India As A Defence Ally
Once the formalities of honouring the late Pope wrap up in two to three weeks time, the conclave of Cardinals will go into seclusion. Some 253 of the current College of Cardinals can take part in the debate over choosing the next Pope, but only 138 of them are below ...4 days ago
- The National Party’s Prison Pipeline Ruining New Zealand
The National Party government is doubling down on a grim, regressive vision for the future: more prisons, more prisoners, and a society fractured by policies that punish rather than heal. This isn’t just a misstep; it’s a deliberate lurch toward a dystopian future where incarceration is the answer to every ...5 days ago
- Don Brash’s NZME Power Grab Must Be Rejected
5 days ago
- 2025 SkS Weekly Climate Change & Global Warming News Roundup #16
A listing of 28 news and opinion articles we found interesting and shared on social media during the past week: Sun, April 13, 2025 thru Sat, April 19, 2025. This week's roundup is again published by category and sorted by number of articles included in each. The formatting is a ...6 days ago
- The “perfect storm” National can use to consolidate slash’n’burn policy is here…
 “What I’d say to you is…” our Prime Minister might typically begin a sentence, when he’s about to obfuscate and attempt to derail the question you really, really want him to answer properly (even once would be okay, Christopher). Questions such as “Why is a literal election promise over ...6 days ago
“What I’d say to you is…” our Prime Minister might typically begin a sentence, when he’s about to obfuscate and attempt to derail the question you really, really want him to answer properly (even once would be okay, Christopher). Questions such as “Why is a literal election promise over ...6 days ago - Economic Futures – Climate Change and Modernity
Ruth IrwinExponential Economic growth is the driver of Ecological degradation. It is driven by CO2 greenhouse gas emissions through fossil fuel extraction and burning for the plethora of polluting industries. Extreme weather disasters and Climate change will continue to get worse because governments subscribe to the current global economic system, ...6 days ago
- Winning Together
 A man on telly tries to tell me what is realBut it's alright, I like the way that feelsAnd everybody singsWe are evolving from night to morningAnd I wanna believe in somethingWriter: Adam Duritz.The world is changing rapidly, over the last year or so, it has been out with the ...6 days ago
A man on telly tries to tell me what is realBut it's alright, I like the way that feelsAnd everybody singsWe are evolving from night to morningAnd I wanna believe in somethingWriter: Adam Duritz.The world is changing rapidly, over the last year or so, it has been out with the ...6 days ago - My Food Bag’s Cecilia Robinson Courts Your Money For Health
 MFB Co-Founder Cecilia Robinson runs Tend HealthcareSummary:Kieran McAnulty calls out National on healthcare lies and says Health Minister Simeon Brown is “dishonest and disingenuous” (video below)McAnulty says negotiation with doctors is standard practice, but this level of disrespect is not, especially when we need and want our valued doctors.National’s $20bn ...6 days ago
MFB Co-Founder Cecilia Robinson runs Tend HealthcareSummary:Kieran McAnulty calls out National on healthcare lies and says Health Minister Simeon Brown is “dishonest and disingenuous” (video below)McAnulty says negotiation with doctors is standard practice, but this level of disrespect is not, especially when we need and want our valued doctors.National’s $20bn ...6 days ago - The Case Against Chris Luxon Remaining PM
Chris Luxon’s tenure as New Zealand’s Prime Minister has been a masterclass in incompetence, marked by coalition chaos, economic lethargy, verbal gaffes, and a moral compass that seems to point wherever political expediency lies. The former Air New Zealand CEO (how could we forget?) was sold as a steady hand, ...6 days ago
- Cameron Slater’s Creepy Fixation On Jacinda Ardern
Has anybody else noticed Cameron Slater still obsessing over Jacinda Ardern? The disgraced Whale Oil blogger seems to have made it his life’s mission to shadow the former Prime Minister of New Zealand like some unhinged stalker lurking in the digital bushes.The man’s obsession with Ardern isn't just unhealthy...it’s downright ...6 days ago
- Fact brief – Is climate change a net benefit for society?
Skeptical Science is partnering with Gigafact to produce fact briefs — bite-sized fact checks of trending claims. You can submit claims you think need checking via the tipline. Is climate change a net benefit for society? Human-caused climate change has been a net detriment to society as measured by loss of ...7 days ago
- National’s Water Done Well Will Cost Ratepayers More
When the National Party hastily announced its “Local Water Done Well” policy, they touted it as the great saviour of New Zealand’s crumbling water infrastructure. But as time goes by it's looking more and more like a planning and fiscal lame duck...and one that’s going to cost ratepayers far more ...7 days ago
- Trump’s Tariff Tantrum Is Causing Economic Chaos
Donald Trump, the orange-hued oligarch, is back at it again, wielding tariffs like a mob boss swinging a lead pipe. His latest economic edict; slapping hefty tariffs on imports from China, Mexico, and Canada, has the stench of a protectionist shakedown, cooked up in the fevered minds of his sycophantic ...1 week ago
- The ‘China’ challenge: now a multi-generational test for Australian strategy
In the week of Australia’s 3 May election, ASPI will release Agenda for Change 2025: preparedness and resilience in an uncertain world, a report promoting public debate and understanding on issues of strategic importance to ...1 week ago
- White Rabbit
 One pill makes you largerAnd one pill makes you smallAnd the ones that mother gives youDon't do anything at allGo ask AliceWhen she's ten feet tallSongwriter: Grace Wing Slick.Morena, all, and a happy Bicycle Day to you.Today is an unofficial celebration of the dawning of the psychedelic era, commemorating the ...1 week ago
One pill makes you largerAnd one pill makes you smallAnd the ones that mother gives youDon't do anything at allGo ask AliceWhen she's ten feet tallSongwriter: Grace Wing Slick.Morena, all, and a happy Bicycle Day to you.Today is an unofficial celebration of the dawning of the psychedelic era, commemorating the ...1 week ago - Why Has The World Forgotten About Hollywood?
It’s only been a few months since the Hollywood fires tore through Los Angeles, leaving a trail of devastation, numerous deaths, over 10,000 homes reduced to rubble, and a once glorious film industry on its knees. The Palisades and Eaton fires, fueled by climate-driven dry winds, didn’t just burn houses; ...1 week ago
- Viennese Refugees Who Changed the Way We Think
 Four eighty-year-old books which are still vitally relevant today. Between 1942 and 1945, four refugees from Vienna each published a ground-breaking – seminal – book.* They left their country after Austria was taken over by fascists in 1934 and by Nazi Germany in 1938. Previously they had lived in ‘Red ...1 week ago
Four eighty-year-old books which are still vitally relevant today. Between 1942 and 1945, four refugees from Vienna each published a ground-breaking – seminal – book.* They left their country after Austria was taken over by fascists in 1934 and by Nazi Germany in 1938. Previously they had lived in ‘Red ...1 week ago - Disputationes adversus astrologiam divinatricem, by Giovanni Pico della Mirandola (1496): A Complete...
 Good Friday, 18th April, 2025: I can at last unveil the Secret Non-Fiction Project. The first complete Latin-to-English translation of Giovanni Pico della Mirandola’s twelve-book Disputationes adversus astrologiam divinatricem (Disputations Against Divinatory Astrology). Amounting to some 174,000 words, total. Some context is probably in order. Giovanni Pico della Mirandola (1463-1494) ...1 week ago
Good Friday, 18th April, 2025: I can at last unveil the Secret Non-Fiction Project. The first complete Latin-to-English translation of Giovanni Pico della Mirandola’s twelve-book Disputationes adversus astrologiam divinatricem (Disputations Against Divinatory Astrology). Amounting to some 174,000 words, total. Some context is probably in order. Giovanni Pico della Mirandola (1463-1494) ...1 week ago - Hamish Campbell Lied About His Links With Two By Twos Cult
National MP Hamish Campbell's pathetic attempt to downplay his deep ties to and involvement in the Two by Twos...a secretive religious sect under FBI and NZ Police investigation for child sexual abuse...isn’t just a misstep; it’s a calculated lie that insults the intelligence of every Kiwi voter.Campbell’s claim of being ...1 week ago
- Is Shane Jones The Most Corrupt Politician in New Zealand?
New Zealand First’s Shane Jones has long styled himself as the “Prince of the Provinces,” a champion of regional development and economic growth. But beneath the bluster lies a troubling pattern of behaviour that reeks of cronyism and corruption, undermining the very democracy he claims to serve. Recent revelations and ...1 week ago
- Good Friday
 Give me one reason to stay hereAnd I'll turn right back aroundGive me one reason to stay hereAnd I'll turn right back aroundSaid I don't want to leave you lonelyYou got to make me change my mindSongwriters: Tracy Chapman.Morena, and Happy Easter, whether that means to you. Hot cross buns, ...1 week ago
Give me one reason to stay hereAnd I'll turn right back aroundGive me one reason to stay hereAnd I'll turn right back aroundSaid I don't want to leave you lonelyYou got to make me change my mindSongwriters: Tracy Chapman.Morena, and Happy Easter, whether that means to you. Hot cross buns, ...1 week ago - Luxon Turns A Blind Eye to Homelessness
New Zealand’s housing crisis is a sad indictment on the failures of right wing neoliberalism, and the National Party, under Chris Luxon’s shaky leadership, is trying to simply ignore it. The numbers don’t lie: Census data from 2023 revealed 112,496 Kiwis were severely housing deprived...couch-surfing, car-sleeping, or roughing it on ...1 week ago
- The Hoon around the week to April 18
The podcast above of the weekly ‘Hoon’ webinar for paying subscribers on Thursday night features co-hosts & talking about the week’s news with regular and special guests, including: on a global survey of over 3,000 economists and scientists showing a significant divide in views on green growth; and ...1 week ago
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}
- Education Should be Led by Experts-Not Economists
Te Pāti Māori are appalled by Cabinet's decision to agree to 15 recommendations to the Early Childhood Education (ECE) sector following the regulatory review by the Ministry of Regulation. We emphasise the need to prioritise tamariki Māori in Early Childhood Education, conducted by education experts- not economists. “Our mokopuna deserve ...2 days ago
- Release: Govt’s flagship cost of living policy a failure
 After promising $250 a fortnight to many families, the Government has been forced to admit just a couple hundred families are receiving it. ...2 days ago
After promising $250 a fortnight to many families, the Government has been forced to admit just a couple hundred families are receiving it. ...2 days ago - Release: Transparency needed on changes to early childhood education
The Government is putting children at risk in early childhood education (ECE) by proposing to loosen the requirement for qualified teachers. ...2 days ago
- Release: Govt funding needed to combat invasive seaweed
The Government must support Northland hapū who have resorted to rakes and buckets to try to control a devastating invasive seaweed that threatens the local economy and environment. ...4 days ago
- New Zealand First Introduces Bill Defining ‘Woman’ and ‘Man’ in Law
 New Zealand First has today introduced a Member’s Bill that would ensure the biological definition of a woman and man are defined in law. “This is not about being anti-anyone or anti-anything. This is about ensuring we as a country focus on the facts of biology and protect the ...4 days ago
New Zealand First has today introduced a Member’s Bill that would ensure the biological definition of a woman and man are defined in law. “This is not about being anti-anyone or anti-anything. This is about ensuring we as a country focus on the facts of biology and protect the ...4 days ago - Release: Labour marks the passing of Pope Francis
Labour Party leader Chris Hipkins joins those mourning the passing of Pope Francis. ...5 days ago
- Release: Boot camps blog post fails to provide clarity
After stonewalling requests for information on boot camps, the Government has now offered up a blog post right before Easter weekend rather than provide clarity on the pilot. ...1 week ago
- Release: Inflation rises and families feel the squeeze
Inflation is rising again and it’s landing hardest on families already stretched thin. ...1 week ago
- Release: Govt doesn’t know how to fund new hospitals
The Government’s health infrastructure plan is big on promises but coy on where the money is coming from. ...1 week ago
- Release: $10 million for only 215 students in charter schools
David Seymour is pouring $10 million into charter schools that only have 215 students enrolled. ...1 week ago
- Release: Food prices further stretching the family budget
Families already stretched by rising costs will struggle with the news food prices are going up again. ...2 weeks ago
- Release: Mental health staff and patients at risk without plan
More people could be harmed if Minister for Mental Health Matt Doocey does not guarantee to protect patients and workers as the Police withdraw from supporting mental health call outs. ...2 weeks ago
- Release: Driver licensing proposal doesn’t put safety first
The Government’s proposal to change driver licensing rules is a mixed bag of sensible and careless. ...2 weeks ago
- Release: Students struggling as Govt sits on hands
The Government is continuing to sit on its hands as students struggle to pay rent due to delays with StudyLink. ...2 weeks ago
- Release: More must be done to stop children going hungry
More children are going hungry and statistics showing children in material hardship continue to get worse. ...2 weeks ago
- Greens continue to call for Pacific Visa Waiver
 The Green Party recognises the extension of visa allowances for our Pacific whānau as a step in the right direction but continues to call for a Pacific Visa Waiver. ...2 weeks ago
The Green Party recognises the extension of visa allowances for our Pacific whānau as a step in the right direction but continues to call for a Pacific Visa Waiver. ...2 weeks ago - More children going hungry under Coalition govt
The Government yesterday released its annual child poverty statistics, and by its own admission, more tamariki across Aotearoa are now living in material hardship. ...2 weeks ago
- Release: Longer wait for treatment under National
New Zealanders have waited longer to get an appointment with a specialist and to get elective surgery under the National Government. ...2 weeks ago
- Ka mate te Pire- Ka ora te mana o Te Tiriti o Waitangi me te iwi Māori
Today, Te Pāti Māori join the motu in celebration as the Treaty Principles Bill is voted down at its second reading. “From the beginning, this Bill was never welcome in this House,” said Te Pāti Māori Co-Leader, Rawiri Waititi. “Our response to the first reading was one of protest: protesting ...2 weeks ago
- Chris Hipkins speech: Treaty Principles Bill second reading
Normally, when I rise in this House to speak on a bill, I say it's a great privilege to speak on the bill. That is not the case today. ...2 weeks ago
- Release: End to the Treaty Principles Bill, but challenges remain ahead for Aotearoa
Ka mate te pire I te rā neiThe bill dies today ...2 weeks ago
- Ka mate te Pire, ka ora Te Tiriti o Waitangi – Treaty Principles Bill dead, Te Tiriti o Waitangi m...
The Green Party is proud to have voted down the Coalition Government’s Treaty Principles Bill, an archaic piece of legislation that sought to attack the nation’s founding agreement. ...2 weeks ago
- Member’s Bill an opportunity for climate action
A Member’s Bill in the name of Green Party MP Julie Anne Genter which aims to stop coal mining, the Crown Minerals (Prohibition of Mining) Amendment Bill, has been pulled from Parliament’s ‘biscuit tin’ today. ...2 weeks ago
- Release: Bill to make trading laws fairer passes first hurdle
Labour MP Kieran McAnulty’s Members Bill to make the law simpler and fairer for businesses operating on Easter, Anzac and Christmas Days has passed its first reading after a conscience vote in Parliament. ...2 weeks ago
- Release: Reserve Bank acts while Govt shrugs
Nicola Willis continues to sit on her hands amid a global economic crisis, leaving the Reserve Bank to act for New Zealanders who are worried about their jobs, mortgages, and KiwiSaver. ...2 weeks ago
- Release: Property Law Amendment Bill pulled from ballot
A Bill to protect first home buyers and others from bad faith property vendors has been drawn from the Member’s Ballot. ...2 weeks ago
- Release: More children at risk of losing family connections
Karen Chhour is proposing to scrap Oranga Tamariki targets which aim to connect more children under state care with family and their culture. ...2 weeks ago
- Release: David Parker made a difference – Hipkins
The Labour Leader today acknowledged and celebrated David Parker’s 23-year contribution to the Labour Party and to Parliament. ...3 weeks ago
- Release: David Parker to step down from Parliament
Long-serving Labour MP and former Minister David Parker has today announced his intention to leave Parliament. ...3 weeks ago
- Release: Flaws in Govt’s climate strategy will cost us money
The Government’s plan to achieve our climate goals falls short, and will cost New Zealanders money and jobs. ...3 weeks ago
- Green Party differing view on the Treaty Principles Bill
Read the Green Party's differing view on the Treaty Principles Bill, prepared by Tamatha Paul. ...3 weeks ago
- 80 years after Benito Mussolini’s death, what can democracies today learn from his fascist rise?
 Source: The Conversation (Au and NZ) – By Matthew Sharpe, Associate Professor in Philosophy, Australian Catholic University Hitler and Mussolini in Munich, Germany, June 18, 1940. Everett Collection/Shutterstock This Monday marks 80 years since Italian dictator Benito Mussolini was killed in an Italian village towards the end of the Second ...1 hour ago
Source: The Conversation (Au and NZ) – By Matthew Sharpe, Associate Professor in Philosophy, Australian Catholic University Hitler and Mussolini in Munich, Germany, June 18, 1940. Everett Collection/Shutterstock This Monday marks 80 years since Italian dictator Benito Mussolini was killed in an Italian village towards the end of the Second ...1 hour ago - Samoan nun tells of ‘like a blur’ awesome meeting with Pope Francis
By Susana Suisuiki, RNZ Pacific presenter The doors of St Peter’s Basilica in the Vatican have now been closed and the coffin sealed, ahead of preparations for tonight’s funeral of Pope Francis. The Vatican says a quarter of a million people have paid respects to Pope Francis in the last ...2 hours ago
- Samoan nun tells of ‘like a blur’ awesome meeting with Pope Francis
By Susana Suisuiki, RNZ Pacific presenter The doors of St Peter’s Basilica in the Vatican have now been closed and the coffin sealed, ahead of preparations for tonight’s funeral of Pope Francis. The Vatican says a quarter of a million people have paid respects to Pope Francis in the last ...2 hours ago
- Reward for revealing netball’s forgotten past
 Once or twice a week, Dr Margaret Henley rolls up the door on a windowless storage locker in central Auckland, pulls her plastic chair up to a picnic table and sifts through the history of netball in New Zealand.She works alongside netball archivist and statistician Todd Miller, together trawling through ...9 hours ago
Once or twice a week, Dr Margaret Henley rolls up the door on a windowless storage locker in central Auckland, pulls her plastic chair up to a picnic table and sifts through the history of netball in New Zealand.She works alongside netball archivist and statistician Todd Miller, together trawling through ...9 hours ago - The secret diary of .. the Dann-Peters interview
Corin DannThe time is 7:36am on Wednesday, April 23, and you’re listening to Morning Report, New Zealand’s voice of the educated left on good incomes. I’m joined now by acting Prime Minister Winston Peters. Good morning Mr Peters.Winston PetersIt was, until I saw you. I much prefer your brother.Corin DannLiam ...9 hours ago
- The ‘atom smasher’ of Auckland University
When Professor David Krofcheck got an email congratulating him on winning the Oscar of the science world, he dismissed it as a hoax.“I thought it was a scam, I thought it was a phishing email,” recalls Krofcheck, nuclear physicist at Auckland University.“Yeah right, I’ve won the 2025 Breakthrough Prize in ...9 hours ago
- The Weekend: The sound of silence
 Madeleine Chapman reflects on the week that was. I’ve been re-watching Girls lately, the HBO classic that perfectly captures millennial women in the most painful way. I highly recommend it especially if you haven’t watched it before. Every character on the show is deeply flawed and frustrating in their own ...9 hours ago
Madeleine Chapman reflects on the week that was. I’ve been re-watching Girls lately, the HBO classic that perfectly captures millennial women in the most painful way. I highly recommend it especially if you haven’t watched it before. Every character on the show is deeply flawed and frustrating in their own ...9 hours ago - When terrestrial television feels like a holiday
With the double-header long weekend comes a welcome chance to escape streaming slop, writes Alex Casey. Over Easter I texted my husband Joe a sentence that perhaps nobody in human history has ever texted: “hurry up geostorm is starting”. No punctuation, no capitalisation, not because I was trying to ...10 hours ago
- The Māori who discovered Europe
April 27 is Moehanga Day, the anniversary of the day in 1806 when Ngāpuhi warrior Moehanga became the first Māori to visit England. This is his story. The wooden ship sailed down the River Thames, past smoke stacks and brick factories, until it reached a wharf in industrial south London. ...10 hours ago
- George Eliot and Daniel Kalderimis and me: on the healing power of Middlemarch
Heidi Thomson on how her husband’s illness and Daniel Kalderimis’s book Zest have enhanced her understanding of George Eliot’s great novel. Sometimes a book finds you at just the right time. In early December my husband John had a stroke. At the time we were both reading George Eliot’s Middlemarch, ...10 hours ago
- ‘Absolutely sending it’: When Marlon Williams partied on the 6pm news
The musician, actor and star of upcoming documentary Marlon Williams: Ngā Ao E Rua – Two Worlds takes us through his life in television. Musician Marlon Williams has been on our My Life in TV wish list ever since he revealed during his My Boy tour that he wrote ‘Thinking ...10 hours ago
- Anzac weekend short story: Toxic, by Michelle Duff
When she walked dripping into the lounge, hair wet from the shower, she took one look at Hamish and dropped her towel.He was holding her phone.—How long has it been going on for?His blue eyes blazed. She wanted to pluck them out and blow on them gently, cool them off. ...10 hours ago
- Kiwi citizens’ assembly succeeds in ‘experiment’ to find climate solutions
A citizens’ assembly of 100 Porirua locals has provided the city council with more than a dozen recommendations about how to tackle climate change and make sure the region is resilient to worsening extreme weather events.Ranging from expanding access to renewable energy and incentivising the planting of native trees through ...14 hours ago
- Mika Hervel: Deliberating on a future for democracy in NZ
Comment: Democracy globally is in crisis. Around the world we are seeing the rise of nationalism and declining trust in democratic institutions. Politicians, even in Aotearoa, undermine the authority of core institutions like the media and the courts, which are critical for a functioning democracy. To live well together, in ...14 hours ago
- Winner of Rod Oram Memorial Essay Prize walks (and rides) the talk
Journalist Rod Oram, who died last year, would have been delighted to see the commitment to addressing climate change shown by the 23-year-old winner of a prize established in his memory.Mika Hervel, a student at Victoria University of Wellington, is today named winner of the Rod Oram Memorial Essay Prize, ...14 hours ago
- Israel’s endgame for tormented Gaza is political and physical erasure
COMMENTARY: By Nour Odeh There was faint hope that efforts to achieve a ceasefire deal in Gaza would succeed. That hope is now all but gone, offering 2.1 million tormented and starved Palestinians dismal prospects for the days and weeks ahead. Last Saturday, the Israeli Prime Minister once again affirmed ...15 hours ago
- Trump signs ‘deeply dangerous’ order to fast-track deep sea mining
An ocean conservation non-profit has condemned the United States President’s latest executive order aimed at boosting the deep sea mining industry. President Donald Trump issued the “Unleashing America’s offshore critical minerals and resources” order on Thursday, directing the National Oceanic and Atmospheric Administration (NOAA) to allow deep sea mining. The ...16 hours ago
- Watch: Luxon’s Anzac Day speeches at Gallipoli, Chunuk Bair
 The prime minister says the name Gallipoli is etched into New Zealand's national identity. ...18 hours ago
The prime minister says the name Gallipoli is etched into New Zealand's national identity. ...18 hours ago - Election Diary: Dutton tops list of most distrusted, amid deepening voter cynicism about political l...
Source: The Conversation (Au and NZ) – By Michelle Grattan, Professorial Fellow, University of Canberra In this election, voters are more distrustful than ever of politicians, and the political heroes of 2022 have fallen from grace, swept from favour by independent players. A Roy Morgan survey has found, for ...20 hours ago
- Pacific editor welcomes US court ruling in favour of Radio Free Asia
By Koroi Hawkins, RNZ Pacific editor The former head of BenarNews’ Pacific bureau says a United States court ruling this week ordering the US Agency for Global Media (USAGM) to release congressionally approved funding to Radio Free Asia and its subsidiaries “makes us very happy”. However, Stefan Armbruster, who has ...21 hours ago
- Watch: Luxon’s Anzac Day speech marks 110 years since Gallipoli landing
The prime minister says the name Gallipoli is etched into New Zealand's national identity. ...23 hours ago
- ER Report: A Roundup of Significant Articles on EveningReport.nz for April 25, 2025
ER Report: Here is a summary of significant articles published on EveningReport.nz on April 25, 2025. Labor takes large leads in YouGov and Morgan polls as surge continuesSource: The Conversation (Au and NZ) – By Adrian Beaumont, Election Analyst (Psephologist) at The Conversation; and Honorary Associate, School of Mathematics and ...24 hours ago
- Labor takes large leads in YouGov and Morgan polls as surge continues
Source: The Conversation (Au and NZ) – By Adrian Beaumont, Election Analyst (Psephologist) at The Conversation; and Honorary Associate, School of Mathematics and Statistics, The University of Melbourne With just eight days until the May 3 federal election, and with in-person early voting well under way, Labor has taken a ...1 day ago
- The Unity Books bestseller chart for the week ending April 25
The only published and available best-selling indie book chart in New Zealand is the top 10 sales list recorded every week at Unity Books’ stores in High St, Auckland, and Willis St, Wellington. AUCKLAND 1 Butter by Asako Yuzuki (Fourth Estate, $35) Fictionalised true crime for foodies. 2 Sunrise on ...1 day ago
- Beating malaria: what can be done with shrinking funds and rising threats
Source: The Conversation (Au and NZ) – By Taneshka Kruger, UP ISMC: Project Manager and Coordinator, University of Pretoria Healthcare in Africa faces a perfect storm: high rates of infectious diseases like malaria and HIV, a rise in non-communicable diseases, and dwindling foreign aid. In 2021, nearly half of ...1 day ago
- The best things from Australia and Aotearoa to watch this weekend
Australia and New Zealand join forces once more to bring you the best films and TV shows to watch this weekend. This Anzac Day, our free-to-air TV channels will screen a variety of commemorative coverage. At 11am, TVNZ1 has live coverage of the Anzac Day National Commemorative Service in Wellington. ...1 day ago
- Lest we forget? The shame of our two-tier veteran system
Our laws are leaving many veterans who served after 1974 out in the cold. I know, because I’m one of them. This Sunday Essay was made possible thanks to the support of Creative New Zealand. First published in 2024. As I write this story, I am in constant pain. My hands ...1 day ago
- Cross-party hope for anti-trafficking legislation
An MP fighting for anti-trafficking legislation says it is hard for prosecutors to take cases to court - but he is hopeful his bill will turn the tide. ...1 day ago
- Bestselling books at Anzac weekend
NONFICTION1 No Words for This by Ali Mau (HarperCollins, $39.99)
 2 Everyday Comfort Food by Vanya Insull (Allen & Unwin, $39.99)
2 Everyday Comfort Food by Vanya Insull (Allen & Unwin, $39.99) 3 Three Wee Bookshops at the End of the World by Ruth Shaw (Allen & Unwin, $39.99)1 day ago
3 Three Wee Bookshops at the End of the World by Ruth Shaw (Allen & Unwin, $39.99)1 day ago - Governor-General’s Anzac Day Dawn Service Address
 This Anzac Day marks 110 years since the Gallipoli landings by soldiers in the Australian and New Zealand Army Corps - the ANZACS. It signalled the beginning of a campaign that was to take the lives of so many of our young men - and would devastate the ...1 day ago
This Anzac Day marks 110 years since the Gallipoli landings by soldiers in the Australian and New Zealand Army Corps - the ANZACS. It signalled the beginning of a campaign that was to take the lives of so many of our young men - and would devastate the ...1 day ago - New Zealand’s role in the mass deportation of Koreans from post-WWII Japan
The violent deportation of migrants is not new, and New Zealand forces had a hand in such a regime after World War II, writes historian Scott Hamilton. The world is watching the new Trump government wage a war against migrants it deems illegal. Immigration and Customs Enforcement (ICE) officials and ...1 day ago
- David Hill: Seize the day
While Anzac Day has experienced a resurgence in recent years, our other day of remembrance has slowly faded from view. This Sunday Essay was made possible thanks to the support of Creative New Zealand. Original illustrations by Hope McConnell. First published in 2022. The high school’s head girl and ...1 day ago
- The Friday Poem: ‘Te Hono ki Īhipa’ by Aperahama Hurihanganui
A new poem by Aperahama Hurihanganui, about the name of Aperahama and Abby Hauraki’s three-year-old son, Te Hono ki Īhipa (which translates to ‘The Connection to Egypt’). Te Hono ki Īhipa what’s in a name? te hono – the connection to your tīpuna, valiant soldiers of the 28th Māori Battalion ...1 day ago
- Daily crossword, Friday 25 April
The post Daily crossword, Friday 25 April appeared first on Newsroom. ...1 day ago
- Newsroom daily quiz, Friday 25 April
Loading…(function(i,s,o,g,r,a,m){var ql=document.querySelectorAll('A[data-quiz],DIV[data-quiz]'); if(ql){if(ql.length){for(var k=0;k<ql.length;k++){ql[k].id='quiz-embed-'+k;ql[k].href="javascript:var i=document.getElementById('quiz-embed-"+k+"');try{qz.startQuiz(i)}catch(e){i.start=1;i.style.cursor='wait';i.style.opacity='0.5'};void(0);"}}};i['QP']=r;i[r]=i[r]||function(){(i[r].q=i[r].q||[]).push(arguments)},i[r].l=1*new Date();a=s.createElement(o),m=s.getElementsByTagName(o)[0];a.async=1;a.src=g;m.parentNode.insertBefore(a,m)})(window,document,'script','https://take.quiz-maker.com/3012/CDN/quiz-embed-v1.js','qp');Got a good quiz question? Send Newsroom your questions.The post Newsroom daily quiz, Friday 25 April appeared first on Newsroom. ...1 day ago
- Open letter to Fijians – ‘why is our country supporting Israel’s heinous crimes in Gaza?’
Pacific Media Watch The Fijians for Palestine Solidarity Network today condemned the Fiji government’s failure to stand up for international law and justice over the Israeli war on Gaza in their weekly Black Thursday protest. “For the past 18 months, we have made repeated requests to our government to do ...2 days ago
- Scares and stunts in the home stretch: election special podcast
Source: The Conversation (Au and NZ) – By Michelle Grattan, Professorial Fellow, University of Canberra Michelle Grattan and Amanda Dunn discuss the fourth week of the 2025 election campaign. While the death of Pope Francis interrupted campaigning for a while, the leaders had another debate on Tuesday night and the ...2 days ago
- Grattan on Friday: Coalition’s campaign lacks good planning and enough elbow grease
Source: The Conversation (Au and NZ) – By Michelle Grattan, Professorial Fellow, University of Canberra Whatever the result on May 3, even people within the Liberals think they have run a very poor national campaign. Not just poor, but odd. Nothing makes the point more strongly than this week’s ...2 days ago
- Inside the elaborate farewell to Pope Francis
Source: The Conversation (Au and NZ) – By Carole Cusack, Professor of Religious Studies, University of Sydney
 View the full interactive version of this article here. Carole Cusack does not work for, consult, own shares in or receive funding from any company or organisation that would benefit from ... 2 days ago
View the full interactive version of this article here. Carole Cusack does not work for, consult, own shares in or receive funding from any company or organisation that would benefit from ... 2 days ago - Nicola Willis confirms FamilyBoost eligibility to be expanded
The Finance Minister says the leftover funding from the unexpectedly low uptake of the FamilyBoost policy will be redistributed to families who need it. ...2 days ago
a shit show waiting to happen
Yeah, the deeper dimension of the pandemic remains a sleeper for now. When the stats solidify, we'll get comparisons between nations emerging. Policy-makers will wait for a pattern to emerge from that, I suspect.
Political parties tend to be averse to representing victims en masse. If there's a third, say, of voters filed into the victim category by long covid, we can expect politicos to notice an opportunity for advantage. First in this race gets the plum!
It's kind of sad that we're still not that good at the deeper, and longer term stuff.
Lol, the crip get a leg in at last!
Good post and yet another reason to pursue elimination or as close to elimination as we can.
Long covid is freaky scary and we just don't know however that will not stop the right banging on about opening up and freedom etc.
Thank my lucky stars we have adults in charge.
really pleased to see the Auckland numbers dropping. Not sure what the government is thinking about long covid, if I had to guess I would say they're probably not really thinking about it (hence the mess Jenene Crossan talks about). Which is not good. Otoh, given the potential impacts, it would be really weird if they weren't taking it into account.
I also count my blessings that we have Labour and not Nat in charge. So lucky.
The govt may or may not be thinking it but pretty sure the health system is.
in what way? I know the MoH has an explainer page up, but from what I can tell they're doing a watch and wait thing rather than putting systems in place.
Victoria University is going to be doing a MoH-funded survey of people who have had covid and what their health and social needs are and their experiences of long covid. I believe it's meant to start in the new year.
https://www.health.govt.nz/news-media/media-releases/study-impacts-covid-19-research-group-contracted
The Spanish flu (which began in Kansas and is another case of misnaming a virus) killed 9000 people in NZ out of a population of about 1 million.
But hidden in the statistics was the on-going health issues which crippled many who survived the flu. Heart disease, lung disease, chronic fatigue and so on. We shall probably never be able to determine how many suffered through the 1920s and into the 1930s.
The precautionary principle is the only logical one for NZ to follow, much as it might upset the Natz and Actoids.
"The World Health Organisation has actually come out now with a clinical case definition for long Covid and it's virtually identical for what is accepted for ME/CFS."
https://www.nzherald.co.nz/nz/covid-19-delta-outbreak-concern-long-covid-will-soon-burden-health-system/2MZREX7IQWZN7CAWELHDZU5O74/
Hell, if clinical case descriptions are identical then you have two categories of victims that ought to be conflated into one! From a public health perspective. If professional treatments & therapies apply to both. Regardless that medical diagnosis and science will separate them into different causal categories.
The Guardian reported last week that there were 750,000 people in the UK with long covid, and that a quarter of these had major life-affecting symptoms
Of course brain fog can be caused by things other than covid (msm, Nat/Lab conferences etc)…
….too much IPA
Nooo not enough IPA.
Evidence to date supports the initial reports that Omicron is a mild infection.
For instance:
10000 Omicron cases in the UK and 7 deaths
https://www.reuters.com/world/uk/uk-reports-leap-10000-confirmed-omicron-coronavirus-cases-2021-12-18/
Also, Omicron seems to infect the upper respiratory tract more, which is one of the reasons why it is more infectious. Also, the virus tends not to attack the lungs as much as previous variations, which is one reason it may be less harmful:
https://www.cnbc.com/2021/12/16/omicron-lung-infection-less-severe-replicates-faster-than-delta-in-human-airways-study.html
Also, it seems that people recover much faster from Omicron than earler variations. The fact it spreads so much faster means it is likely to burn out much more quickly as well.
There are two main worries with the virus. Firstly that it will overwhelm health systems by weight of numbers, despite being less harmful. The results from the UK don't seem to be supporting that concern at the moment.
The second concern is that there could be severe disruption due to so many being sick at the same time, even if they don't need hospitalisation. This may eventuate to be the main problem, but hopefully a short-term one.
It will be a good thing if the virus turns out to be quite benign, doesn't cause undue disruption, and helps build natural immunity to other more harmful versions that may arise.
how does that relate to the post? Did you read the post?
I guess the point, that I didn't directly mention, is that Omicron may be a lot less likely to produce long-Covid because it doesn't seem to be as damaging to other organs, the lungs anyway.
As you mention, possible cause for long Covid is that the virus can leave persisting damage that takes a long time to heal.
https://www.bbc.com/news/health-57833394
If Omicron is less likely to do that, and if Omicron becomes the dominant strain, then long Covid may become very infrequent going forward.
'may' being the operative word in your first and last sentences, hence the need for the precautionary principle. I don't want us to take the gamble.
I guess the advantage we have is that we are going into our summer when bugs don't tend to spread as much, and we have time to assess what is going on with the Omicron virus.
Eventually viruses do tend to become less harmful over time. The common cold was probably once a deadly pandemic.
We really need Covid to mutate into a much lower level disease because I think that is ultimately the way out of this.
From what I have read, the most common symptoms of Omicron are very much like the common cold, and sound boringly familiar, eg:
https://www.irishmirror.ie/news/expert-lists-five-most-common-25737028
They only become less harmful “over time” by killing off a generation of people in Darwinian fashion
It has already done that.
One of the explanations for Omicron not being so harmful is that most in the world are now vaccinated or have had Covid already. So immune systems worldwide recognise Omicron much more quickly and fight it off more effectively.
Problem is it doesn't show if it is killing vaccinated or unvaccinated.
The other is because it's spreading faster with quicker infection period it could infect many times more people leaving many more dead.Until those figures come out nothing can be taken for granted.
NZ has time to disseminate and prepare..
Brian May "Queen "guitarist and his wife both caught covid after booster doses and said they were very ill and don't take covid for granted.
and even if the death (or hospitalisation) rate is lower, even much lower, we also don't know the long covid rate. Or what comes after omicron.
The people advocating for let it rip/herd immunity are advocating for more death and disability or at least saying let's take the chance. It's not a button we can unpush.
Well said Weka
One of the good things about Omicron spreading so quickly is that the effects are also known much more quickly.
If this turns out to be a relatively benign illness we will know quite soon I expect.
If it is true that it causes very little harm, probably the best thing that can happen would be for it to arrive and run through the population.
It seems to be the course that Australia is taking at the moment.
https://thewest.com.au/news/coronavirus/victoria-nsw-drive-record-covid-19-cases-c-5004936
So it will be interesting to see how that turns out for them.
how long will it take to establish whether omicron causes long covid?
There will likely be decreasing occurrences of long covid and other negative outcomes with any Covid mutation that comes out due to the much higher vaccination rates and natural immunity around the world now.
If Omicron is indeed a much milder version, then, that factor as well should reduce the incidence of long Covid, as it would be less likely to cause lasting damage to organs.
That is not to say that long Covid would never occur. But it should be far less frequent due to both factors above.
“likely”
”should”
do you think it’s wise to base public health policy on guessing?
They are appropriate words to use when discussing something none of us are sure about yet.
Do you think there would be any point to future lockdowns of the nature we have endured recently should Omicron take hold?
If it is as contagious as it seems to be, then lockdowns would have to last a long time in order to be effective. A "short, sharp, circuit breaker" would only delay the inevitable for a few weeks. And I don't know if the public would put up with long lockdowns now. I think there would be mass civil disobedience were the government to head in that direction again.
What are your thoughts on that?
I think any analysis that doesn’t overtly take long covid into account is virtually useless.
I also think that omicron is still so new that we don’t have enough information to be basing decisions or even theories on.
that was the point of the post. All the angsting about lockdowns and borders is missing the point.
Ohio whose hospitals are overwhelmed at the moment, the health workers took out a full page ad with the word HELP on it, is saying that while you are 4 times less likely to be hospitalised from Omicron you are more than 4 times likely to get it.
While Omicron cases haven't really hit them yet they are dreading what is coming. They are also expecting more healthcare workers to get sick than previously due to the higher infection rate.
National Guard is being called in to do testing as health workers have moved to the front-line.
https://twitter.com/njKaitlinDurbin/status/1472713083126792195?ref_src=twsrc%5Etfw%7Ctwcamp%5Etweetembed%7Ctwterm%5E1472713083126792195%7Ctwgr%5E%7Ctwcon%5Es1_&ref_url=https%3A%2F%2Fwww.wkyc.com%2Farticle%2Fnews%2Fhealth%2Fcoronavirus%2Fohio-hospitals-help-plea-covid-surge%2F95-d877d2e3-c65b-4fa1-8df6-70a424a394c7
Everyone seems to be afraid it that Omicron will overwhelm health systems. But I am not sure there is evidence of that actually happening yet.
Bit early yet as it moves through the population in the US and UK The first deaths are just starting to happen.
Also will likely be a bit less dangerous as many of the most vulnerable have already died in many countries. They can't die a second time.
90% are double vaccinated in New York, the population is scrambling to get the booster. The unvaccinated group are more representative when it comes to hospital admissions.
Cases of Omicron double every 2 – 3 days. See what the situation is like in a week in New York.
I expect an Omicron community case in NZ before the New Year.
As for long Covid due to a shortage of scientific and health resources this is not being looked into how it needs to be.
It's too early to tell, omicron has been around for 2-3 weeks – for delta it takes a week or two to make it into hospital, then a few weeks to die, such is modern medicine, we really don't know yet how good or bad omicron is going to be.
Saying that it's mild is frankly wishful thinking (I'm guilty of doing this). One of the problems with covid compared to previous epidemics is that because of modern medicine (both vaccines and hospital treatment) most people survive – that means that the evolutionary pressure that killing off your host presents is absent, there's no reason for it to get milder as the epidemic moves onward.
ooph, that last bit is a kicker.
It's too early to tell, omicron has been around for 2-3 weeks
Actually a fair bit longer than that, but hey….
The evolutionary pressure that could end very badly comes from a universal roll out of leaky vaccines (reference Merak's virus).
And a virus that has "jumped ship" before a host dies isn't impacted by the death of a host. Jist sayin'.
Bill hopefully
But also more hope reading through your link yesterday
re:headline,Denmark omricon out break affecting 89.6% of double vaccinated and booster shots infections.
80% of new infections were double dosed While only 10.3% of new infections were triple dosed/booster shots.Hopefully this figure continues to show a trend. And may hurry the end of Covid .
Jus saying.
Have a close friend with CFS and it’s no joke. She can only do low level activities for a few hours a day. Spends a lot of time resting while her body furiously burns up all her energy
Yesterday I posted about sufferers of CFS/ME desperate for Covid vaccine exemptions because of the 1 in 4 chance that the vaccine will trigger a severe relapse of their symptoms. They are desperate …but the MOH in their infinite wisdom and compassion just says that they should wait until they recover from the (severe) reaction from the first shot before have the second.
The same comment also included a link to a very interesting discussion between Kim Hill and a Kiwi member of the WHO SAGE panel. Well worth a listen, and at around 28 mins he claims that Long Covid is not as common as was first suspected and that being vaccinated makes it much less likely. As an expert advisor to the WHO, and a down to earth Kiwi, he should know a thing or two.
And finally…while searching for some information about heart and pain issues in a 30 year old relative after her having the second shot back in June, I stumbled across this site… https://vestibular.org/forum/dizziness/covid-19-vaccine-side-effects/
This site has been around for some time, and offers advice and support for people managing vestibular dysfunction. This particular thread on their forum began in January this year as the vaccines were being rolled out in the US. I read page after page of that particular thread ….and the symptoms described so closely echo that of ME and Long Covid it is unnerving. Some of those posters say that they were just getting over Long Covid when they had a vaccine that set them right back again. A few of the posters are from New Zealand and Australia. Far too many expressed a desire for an end to their pain.
Because over and over they tell how the medical system, and the general public has treated them with disdain and dismissal. Just like the sufferers of ME endured here in NZ in the eighties.
So we are looking down the barrel of two groups of Covid damaged weka…those with Long Covid from having the disease, and those with post Covid vaccine syndromes.
FWIW…reading those posts (up to about page 500 before I became too depressed) and I came to realize that many of the symptoms described matched what I had been experiencing since May last year. More than one WTF!!! moments to be sure. No test for Covid, but the most awful dizziness (I've had this before, but not as bad), sudden exhaustion, heart 'flutters' ,extreme bone aches and periodic brain fog. I developed a very sudden intense sick making reaction to tea. The smell and the taste of it. A lifetime tea- swiller, I haven't managed a sip since.
This is why I will not be having the Pfizer Product. I am feeling much, much better after starting to take Vit D3. (Yes, me too.) Heart flutters gone, dizziness mostly gone, brain fog gone, and I added Vit K a month ago and the horrible bone aches have much improved. (Just as well , as the very probable hip replacement in my future will be a no go as we Fucking Filth unvaxxed will not get a look in.)
I personally would not trust either MOH or MSD to step up and provide the support that will be needed. We really need to be doing more to help ourselves and each other into the future.
I think this is likely too, although to what extent people with chronic illnesses are getting a new syndrome or a flare of an existing one, we don't know. And probably won't know because the research is going to take a long time or not happen at all.
I'm glad things have shifted in TS a bit so that at least we can talk about this. Much of the year of seeing people saying that there were no concerns about the vaccines when anyone listening to the experiences of disabled people knew that there were. We've still not had that conversation here fully, it's one of the worst examples of prejudice and ableism I've seen here.
The problem is that we don't actually know. My guess is that the down sides of the vaccine will be outweighed by the reduction in covid death and disability, and PTSD and burnout in the health system. I chose to be vaccinated because my life is hard enough without having to deal with vigilance once covid arrives here (I consider myself at risk, and so does my GP, despite the fact that the MoH doesn't lol). And yes, the mandates were part of that decision too. I also want to be able to spend time with elderly relatives.
The naivety around the MoH and how mainstream medicine treats disabled and chronically ill people is sometimes just too much to deal with. I think lots of people are in for a wake up call over the next year or so. Maybe we will get lucky with omicron, maybe not. Time will tell.
I am so glad that you are feeling better and that you found out what worked for you. Again, the science heads can pontificate all they like about RCTs, meanwhile there are whole subcultures out there figuring stuff out for themselves.
Yeah, I don't really trust them either, but wanted to leave something hopeful open in the post. Completely agree with your last sentence. Unfortunately I'm nearly as cynical about the ability and willingness of people to help each other as I am about the MoH/MSD. But please keep talking about that aspect, I'm totally open to changing my mind.
btw, can they not test for past covid infection?
btw, can they not test for past covid infection?
Until fairly recently no. Now…last I heard it was between 75 and 400 dollars. Hard to get a Doctor's refferral.
Been a common topic of conversation around these parts as to whether there was Covid going around…late 2019 to mid 2020…with a fair number of folks describing similar symptoms. Especially a persistent post 'flu' cough. My extreme dizziness…a neighbour took a guest of hers to the doctor for the same thing the same day I had a particularly bad turn. Weird. We (very jokingly) blamed it on the nearest cellphone tower.
Spoke to a local woman whose husband and brother died from a particularly nasty chest bug type thing when they lived in Ausssie in late 2019.
Who knows…I reckon it pays to keep a very open mind.
https://www.newshub.co.nz/home/new-zealand/2021/03/coronavirus-likely-there-was-undetected-transmission-of-covid-19-in-new-zealand-in-early-2020-experts.html
I've heard that thing about Italy having covid in late 2019. It begs the question of why clusters didn't form. Or if they did, there were no deaths and so they weren't investigated. Maybe low numbers and a slow spread at the start?
Northern Italy has strong connections with China.
The Car industry,Fashion,electronics and software.Many travelling back and forward for work related reasons. Also Italy is a big destination for Chinese tourists.
(Conspiracy alert!) Remember all those odd pneumonia deaths in the US that were slated back to vaping? They happened around Fort Detrick – a bio research lab that the federal government shut down because "safety protocols".
Then there was an international games event in the Wuhan region….
I'm glad things have shifted in TS a bit so that at least we can talk about this.
All the evidence points to our medical establishment comprehensively failing to deal with the 'diseases of civilisation', or 'living indoors'. Before COVID we've already had on-going crisis with cancer, diabetes, cardiac disease, obesity, ME/CFS, autism, anxiety and depression and more. All diseases that were once relatively rare in our grandparents generation – now commonplace. And many of them implicated as so-called 'co-morbidities' with COVID.
The link could scarcely be more obvious, nor more relevant to public health than ever before. It’s my view that Long COVID is but one more illness that arises in the same constellation of chronic diseases the naturopaths and functional medicine people have been talking about for decades.
yep.
Here's part of the problem. Many mainstream people simply don't have the literacy to understand how alternative or holistic health works. And many alternative types don't have the scientific literacy to understand where the limits of alternative health lie.
Hence we have people believing that their organic diet will prevent them from getting covid, rather than it (probably) offering some protection but many organic diet (or whatever) people will still get covid and some will die/get long covid.
Hence we have a mainstream medical profession incapable of doing research on large swathes of stuff that works.
Ideology blocks understanding in both cases.
I think the alternative sector will develop a lot of really useful stuff about managing pre-hospitalisation covid in the next five years (almost certainly the Chinese have been doing this for the past 2 years building on previous respiratory events, and they are much better at integrating TCM and Western medicine). But the inability to document that along with the FB-isation of knowledge means that we won't get really good information separated out from the shitty/useless stuff.
Outside chance we might get a paradigm shift that will change both those cultures.
Does Delta cause long Covid? Yes.
Covid is endemic. It's not going away. It is not possible to vaccinate a way out of an endemic situation with leaky/non-sterilising vaccines.
So there's that.
Does Omicron give rise to long Covid? Maybe.
Is Omicron worse than Delta in terms of the immediate effects it has? I think we can safely conclude from overseas, on the ground data, that it is not worse than Delta. Quite the contrary, it would appear to be much, much milder.
So there's a potential to save lives by having Omicron displace Delta as the dominant variant – which it is doing anyway. Or we could hang on to "the devil we know" for as long as we can, and possibly cause more death and more debilitating illness (both from infection and new rounds of mandated injections) than would otherwise be the case.
Maybe Omicron will produce far worse and far more long Covid than Delta and injections currently do. Thing is, that's an unknowable, and so can't be a part of any rational decision around which variant we'd rather be subjected to.
There are times for precaution, and there are times to act. This is one of those times.
what's the evidence that omicron will displace delta and that we won't have another variant that is worse?
I don't see the rationale for acting in the way you are suggesting. We don't yet know what the long covid rates will be. We don't know if letting widespread community transmission will create new worse variants.
The current slow strategy is about flattening the curve as much as anything. The government is no longer pursuing elimination. Flattening the curve brings a lot of benefits (less PTSD and burnout for staff, less flow on effects to the health system, less deaths if the hospitals get overwhelmed) as well as giving us time to see how the whole thing is developing.
The precautionary principle should be part of any rational decision making process. It's not that we know nothing. What you are suggesting is we press a button that we can't unpress, and if we get it wrong it could have catastrophic consequences. That's a gamble, roll of the dice kind of thing.
what's the evidence that omicron will displace delta and that we won't have another variant that is worse?
It's a logical outcome well understood principles of evolutionary biology – the variant that replicates the best will always dominate a population. We've seen this in action as Delta rapidly replaced all the previous letters of the Greek alphabet wherever it showed up.
The other more subtle idea is that there is usually an evolutionary trade-off between infectiousness and lethality. In the specific case of Omicron it appears that it infects the bronchial tracts very rapidly, much faster than Delta, which explains why it's breathed outward very readily. This must form part of the explanation of why it's so transmissible. Yet it's much slower at infecting the alveolae which means in principle it should be less lethal.
Campbell gave a lot of detail on this just today.
All virus's care about is reproducing, there is no evolutionary advantage to killing their host. Which is why we've rarely had to face the nightmare of a naturally evolving virus that is both highly lethal and transmissible.
If we combine these two broad principles together with what we already know about Omicron, the reasonable expectation is that it will rapidly dominate and eliminate all other variants. And at the same time confer an additional immunity, over and above vaccination, to the entire human population all within a timeframe we could never achieve ourselves.
There remains the open possibility of future variant that is even more transmissible, but again in principle the chances of it being also more lethal than say Delta are fairly low. After all we've already lived with the common cold – another very transmissible coronavirus – for a very long time without this happening.
It's not that we know nothing.
True. We know that the severe illness and death rate from Delta is higher than that from Omicron.
We know there are deleterious consequences and death associated with injections.
And we could stack up the numbers in the ledger and make a decision that way.
Delta + booster = ?
Omicron + no more injections = ?
Just a thought.
https://www.aljazeera.com/news/2021/12/18/no-evidence-omicron-milder-than-delta-british-researchers-say
Early days but Omicron might not be as weak as you think Bill.
How deadly a mutation appears depends on the people who are catching it. If only young people are catching it then it's going to look less vicious then if it was a group of older people catching it.
The thing with a virus is that it spreads through peer groups so groups of people with the disease aren't random samples of the population. You have to be very careful with generalising cases to the entire population.
The problem is the potential for a leaky vaccinated environment to favour a more lethal dominant variation that would have 'bitten the dust' if we hadn't messed with the viruses environment in the first place. (So, why keep vaccinating as “a matter of faith”?)
Look up Marek's virus for a parallel situation.
Which is why we've rarely had to face the nightmare of a naturally evolving virus that is both highly lethal and transmissible.
See what I did there?
Thankyou Weka for doing this post about Long Covid, which sounds real similar if not exactly the same as ME. I am double jabbed and still wondering if my ME has gotten worse. Certainly I feel a bit worse but such is the disease you can not be sure because summer/heat does this anyway, for me.
I believe without the vaccine protection I would be very badly effected by Covid and my body simply would not cope with both. I have read that the ME Society is reporting some members are relapsing or experiencing significant worsening of their ME after the vaccine. That's a big bummer for them for sure. I must be lucky?
37 years I've had ME and counting. That's the thing, it' never ends. There is no cure and the medical profession don't want to know. They know zero about it. Covid is one thing, but ME will make you feel like shit for the rest of your life. You don't want it.
Thanks again Weka keep up the good work.
37 years I've had ME and counting. That's the thing, it' never ends.
I'm sincerely sorry to read that.
Thank-you GreenBus, much appreciated. I hope your symptoms settle down again soon.
It's so frustrating that health authorities have basically left chronically ill people to sort this stuff out themselves.
From what I can make out (not the best at navigating these supposedly interactive sites) – 0 new cases in S.A. over the past 24 hours.
https://gis.nicd.ac.za/portal/apps/opsdashboard/index.html#/15eb33988f104b73867606c1248578ff
I agree with the post.
Medical science is bloody good at dealing with stuff it can test for.
Omicron was first detected less than a month ago. In that time it's been identified, genetically sequenced, its extent largely tracked, and research is well underway looking at its characteristic symptoms. We know what it had for breakfast. This is star trek-level shit compared to thirty years ago. That's the "yay!".
But if there's, say, a month lag from infection to hospitalisation with this one, there might not have been enough time to identify that change. If it affects some demographic more than others, it might not have hit those groups of people yet in any great number. Numbers around vaccine efficacy, variant dominance, morbidity and mortality are all still a bit fuzzy at the moment. If it has half the mortality rate but five times the transmission rate (but maybe with a wider window), that's worse. A tenth the death rate and twice the transmission rate – still bad, but possibly better than delta. We don't know yet, though. Reports of the benevolence of our possible new overlord are grossly premature. That's the "hmmm, still not happy" bit.
Where modern medicine does have a habit of falling down at individual and systemic levels is dealing wioth things that can't be identified on a machine that goes "bing!". CFS/ME, back pain, any pain without an obvious associated injury/issue – anything patient reported is still subject to the biases and the ignorance of people in the system. That's the "houston" call.
For example, the wikipedia long covid page has oodles of buts, ifs, and maybes in it. The omicron page has a picture of its damned family tree right up top.
Diabetes is fine – blood test reaches some level, they throw pills and courses at you. Heart disease – blood pressure, various scans, no problem. Badly broken bones have xrays, and cuts have red stuff coming out. But fatigue? Pain? Stiffness? Subjectively reported, and subjectively observed and recorded. Doc has a bad day, or a bias, or doesn't want to touch that area? Who knows what might be put down. Those records create preconceptions in the next people in the system. "Hysteria". "Malingering". "Difficult patient".
So my point is that if long covid doesn't have something clear to test (or the least impactful symptom has an easy test but the most impactful symptoms don't), the true extent and severity of it will take a darn sight more time to nail down than simply identifying the virus behind a sudden massive surge in respiratory hospitalisations. And that will have the flow-on effects through the way governments choose to (not) provide additional support. Which will hit poverty levels as people lose work because they can't do it.
It's an if. But even without the if over omicron, long covid will take a while to clearly put together.
that's an incredibly good description, thank-you McFlock
The sceptic in me says the medical experts have no tools in the toolbox for long covid, no test results other than "your normal" come back and see me in a week. Sell you a lot of pills though, see if anything works? Then give up. Yep that's ME all right. This has been happening in the UK, a lot. Like you say McFlock if they can't test for it your shit out of luck. There is help out there but not from your GP and attached Specialists.
Your job is to find him/her and for that you will need help of family or friend.
Your GP will be glad to see the back of you so your on your own. Look alternative and try the lot.
Long Covid – a non-medical term – would probably be better named undercared-for chronic suffering. That's because there are various names for long Covid (post-intensive care syndrome, chronic Covid syndrome, post-Covid-19 syndrome, and post-acute Covid-19) and because other viruses can also have serious long-term effects.
But the same problems exist for affected patients that the medical profession has mistreated and disbelieved over many years.
https://www.vox.com/22298751/long-term-side-effects-covid-19-hauler-symptoms
Covid is an endothelial disease. Endothelial disfunction is fingered in cardio-vascular disease, CFS and arthritic conditions among others.
https://academic.oup.com/eurheartj/article/41/32/3038/5901158
https://twitter.com/EmmaVitz/status/1472997125315309576
The sceptic in me says the medical experts have no tools in the toolbox for long covid, no test results other than "your normal" come back and see me in a week. Sell you a lot of pills though, see if anything works? Then give up. Yep that's ME all right. This has been happening in the UK, a lot. Like you say McFlock if they can't test for it your shit out of luck. There is help out there but not from your GP and attached Specialists.
Your job is to find him/her and for that you will need help of family or friend.
Your GP will be glad to see the back of you so your on your own. Look alternative and try the lot.
From the UK (20th December):
https://news.sky.com/story/covid-19-scientists-surprised-by-properties-of-omicron-variant-says-nervtag-expert-12500712
From the article:
In Britain, 12 people infected with Omicron have died, while 104 people with the variant are in hospital, according to latest figures from the UK Health Security Agency.
This is from a population of over 50 million.
As mentioned above, the article is from the 20th of December, so covers a few weeks over which Omicron has been circulating in the UK.
That only 12 have died thus far, and only 104 people in hospital is not consistent with the proposition that health systems are in danger of being overwhelmed.
Granted, we are still early in this, but surely there would have been a much greater impact in the UK by now if Omicron was that bad.
Your ‘surely’ is a bit daft and doesn’t show any conception of the basic logistics or compounding with large numbers.
Generally with covid-19 it has taken about 5 days to go from infection to symptomatic, and about 5-12 days from symptoms to requiring hospitalisation where the services have existed.
The infection to symptoms with omicron has been shorter – probably 2-3 days. No-one has any real idea about the hospitalisations rate. It usually takes days to weeks thereafter to die depending on how long they waited before admission..
Ok – lets say that is 7 days lag to hospital and 14 days lag to death.
Then what we are seeing is just what happened to the people who were infected right at the known community transmission.
Now consider that omnicron has a rough doubling rate of about 2 days. Makes it easy for those of us who do binary numbers.
start at 1, double every two days
2, 4, 8, 16, 32, 64, 128, after 14 days of doubling (ie probably about when community was noticed in teh UK.)
256, 512, 1024, 2048, 4096, 8192, 16384 is what you get after 28 days (probably roughly where they are now).
32768, 65536, 131072, 262144, 524288, 1048576, 2097152 after 42 days (where they will be in 2 weeks)
Well what do you know 2 million odd in 40 odd days. According to you only having a few hospitalisations amongst the first few weeks of known infections be infected is ok. What happens in a few weeks of exponential growth?
Please learn to think about numbers before you do any more of these completely stupid reckons. You sound as thick as Mike Hosking.
Actually I do understand the numbers. But, this virus simply does not seem to be having the same effect as previous versions. So I have cause to be optimistic. Though I have said a number of times, it is still early days, and we will have to see how things play out around the world.
For instance, the US has only just recorded its first Omicron death. This despite Omicron now comprising 73% of cases.
https://www.ndtv.com/world-news/coronavirus-unvaccinated-texas-man-becomes-first-omicron-death-in-us-report-2662334
Also, on TV1 News tonight, it looks as if Omicron cases have peaked already in South Africa, with case numbers now dropping, despite it only becoming a thing a few weeks ago.
I agree with the government keeping the borders closed for longer so we can see what is happening world-wide and shore up our vaccine readiness.
After that, I don't think there is much point trying to keep it out, and we should just accept the inevitable.
I don't think we can keep it out.
But we do need to throttle the number of sources of import (ie the start points of the geometric progression) for the moment until we do understand how it spreads and what effects it has on the medical system.
Looks like the government has pushed everything out for about a month – seems about right. Let SA, UK, USA and Aussie test it for us.
It’s the ratio between infections and death/disability that matters, not overall population. And the time lag for both acute crisis and then long covid. Two weeks is nothing.
Granted, that several weeks isn't long. But, the Omicron virus also develops much more quickly, and people recover much more quickly as well.
However, Omicron is just days away from becoming the dominant strain in the UK, and has already done that in a number of countries, including the US.
https://www.independent.co.uk/news/uk/boris-johnson-london-omicron-prime-minister-people-b1975105.html
Given that Omicron has now become so dominant, we should start seeing the impact on health systems very quickly. Thus far, there doesn't seem to be any indication that is happening. Though things could change.
It looks like most people start recovering from Omicron after 3-5 days:
https://www.birminghammail.co.uk/news/health/how-long-omicron-symptoms-last-22478317
This much shorter recovery time is consistent with the proposition that Omicron is much less severe, and therefore, less likely to cause the damage associated with long Covid.
Another important point is that faster recovery could well mean much shorter stays in hospital. So, even if the same number of people end up in hospital compared to Delta, if their stay is shorter, beds become free much sooner.
I am hopeful the most optimistic scenario will be the actual course of Omicron. Time will tell fairly quickly I think.
Omicron or no I suspect those working in NZs under resourced health system are ready for some respite….the real question is are the wider population ready and willing to change the settings to enable necessity over wants?
Voting patterns suggest not yet.
Voting patterns suggest not yet…
The Herald is running a poll...Do you agree with delaying New Zealand's border re-opening?
Yes…..36%
No……64%
From an article headed….'Crushing the souls of Kiwis': Tourism industry, airlines and Kiwis abroad react to border delay
There's clearly an appetite for 'let it rip'. A bit silly by my reckons…we are comparatively Covid naive here…unless there have been a tonne of undetected cases and we have a more natural immunity than we think.
Curious how single issue polling results are seldom reflected in elections.
It seems to me to be a continuation of the theme 'somebody else' can do the work.
This is probably one of the most important and aware posts I have ever read on The Standard.
For someone who has suffered from a "complex medical history of symptoms" pre covid for over 35 years and in more recent years has struggled to even see a specialist under the public health system your concern for those who are now enduring long covid addresses for me the elephant in the room.
Our highly conservative PHS has neither the tools nor the awareness nor central government enthusiasm to act in the best interests of this as yet unrecognised tidal wave of long covid community.
My partner and I have over the years lost faith in Big Pharma and we have both led a healthy and holistic life but genes and early childhood exposure to DDT and 245T (dairy farm) have caught up with me but at a much earlier age than could ever be anticipated.
If only the awareness (mostly) that I am experiencing in this post and the resulting comments could be transferred into the wider community. But everything about covid 19 has been polarising.
Instead of being united in a global response to research, funding, economy and most important politically we have failed the greatest test (medically) humanity has faced for over a hundred years.
You are right Weka to highlight the lack of awareness over long covid but the system we live in is not prepared to react satisfactorily or with equity.
A sense of privilege, greed, entitlement reigns chillingly over the well meaning and socially progressive thinkers and doers.
The tragedy and travesty we are witnessing over the detention of Julian Assange after he dared to speak truth to power is testament to how far we have fallen as a society.
Again I have to congratulate you Weka on firstly raising the issue of long covid but having the ability to enunciate with empathy.
Also the many comments from people who understand (for those card players)some of us are just not holding a good hand.
pukahu road – your exposure to DDT and 245T is similar to mine. High levels of Roundup were found in my system by several alternative practitioners. From age 20 sprayed a lot of Roundup around an orchard in the BOP, with out any protection. Told it was safe. Age 22 out of the blue got the "Tapanui Flu" or ME it's proper name.
A Reflexology practitioner in TGA purged most of it out of my system in 6 months of treatment. A 50% improvement. Yee Ha. That was mid 80's, still got the other 50%.
I took a keen interest in Dire Straits new song "Industrial Disease". Makes you wonder what chemicals do? Mainstream medical no help at all.
Well that says a great deal and well worth saying.
Our highly conservative PHS has neither the tools nor the awareness nor central government enthusiasm to act in the best interests of this as yet unrecognised tidal wave of long covid community.
And not just long covid – but a whole constellation of chronic 'diseases of civilisation'.
My partner and I have over the years lost faith in Big Pharma and we have both led a healthy and holistic life but genes and early childhood exposure to DDT and 245T (dairy farm) have caught up with me but at a much earlier age than could ever be anticipated.
My partner and I are also in that place.
2008 saw our dairy farmer neighbour in the Waikato have his farm (sharing three borders with out little acre) helicopter sprayed with what we were assured by the Waikato Regional Council was a harmless spray for facial eczema. When my partner was diagnosed with Hairy Cell leukeamia two years later we embarked on a journey that ultimately led to our complete disillusionment with The System. We have no doubt the spray caused the leukaemia, and are reasonably sure we understand why my partner developed it and not the rest of us.
Theoretically, HSNO products are permitted for use (after an approval process that largely hinges on manufacturer's information…ring any bells re the Pfizer product?) under supposed strict conditions designed to protect the user and others from serious adverse effects from off target application.
Sounds awesome if those conditions were rigidly enforced. Or even acknowledged as being expected by those using these chemicals. And as for trying to get the regulatory authorities to do their job and protect people from the serious adverse effects of off target application…forget it. And trying to get the local Public Health officer to step up and recognise that this particular chemical, banned in other countries and certainly not permitted to be sprayed from helicopters, was a wasted effort.
And on the Haematology waiting room wall there was a laminated article about a rural couple who both had leukaemia and sprays were suspected. When we told the registrar we believed my partner's leukaemia was caused by an agrichemical we were totally dismissed. The cause of the disease was of no interest…
Conventional medicine helped…but we very quickly realised we needed to explore 'alternative' ongoing therapies that supported the body's natural ability to repair and rejuvenate.
I'd like to think there could be some real change in the future…users of agrichemicals would respect others' right to not be poisoned, the authorities would make sure they followed the rules every single time the sprays were used and if there were breaches of the Rules then all hell would rain down upon the reckless.
I'd like to think that the medical establishment will become more interested in the causes (and prevention) of disease in the future as it become more obvious that Big Pharma not only does not have all the answers but are raking in huge profits by making many people sicker.
But I won't hold my breath.
huh, thanks for that, that actually helps me understand your feelings about the covid vaccines better.
My own chronic illness came from other things, but I had a close relative whose health collapse from probably ag chem exposure. It's nasty. Have known an Agent Orange survivor too.
For me, most of the ag chemicals are unnecessary. We already know how to grow food without them, they are instead about profit and convenience. People getting ill are collateral damage from that, imo this is insane when we could be using mostly organic and regenag. I don't think it's even about using them correctly, because if we protect humans we're not protecting the rest of life, and that's us too.
The vaccines for me are different. Not because we they don't cause problems, but because we have few other options right now.
thank-you pukahu road, that's very gratifying.
Like you and others, my main way of managing long terms has been mostly outside of mainstream medicine. I feel a mix of angst and compassion when I see so many people, especially younger people, getting long term illnesses and being completely dismissive of alternative or complementary medicine. This comes from bad experiences perhaps, but also philosophical positions. And definitely because mainstream medicine has had its head up its arse pretty much the whole time when it comes to things that work that it won't understand. Blows my mind that we still don't integrate the two systems.
https://www.independent.co.uk/news/uk/boris-johnson-london-omicron-prime-minister-people-b1975105.html
It is looking like Omicron has already peaked, and there has been no increase in hospital admissions.
Also cases have dropped by 40% in South Africa a month after Omicron being detected:
https://metro.co.uk/2021/12/21/south-africa-covid-cases-fall-by-40-a-month-after-omicron-first-detected-15802847/
So, it looks like there is little to fear from Omicron, and that given the benign effect, long Covid may not be a huge problem either.
Has Omicron become OmiCON?
I wouldn't put money on it, Pollyanna.
https://twitter.com/chrischirp/status/1473362907471699979
https://threadreaderapp.com/thread/1473362907471699979.html
Yes I know it is early days, and things may change.
But wouldn't it be great if I am right?
It is interesting to look at earlier predictions for instance, four days ago an expert predicted cases would peak in January:
https://www.mirror.co.uk/news/uk-news/omicron-cases-peak-january-new-25643415
But now it looks like they have already peaked, and could even start declining in the coming days:
https://www.dailymail.co.uk/news/article-10333125/Covid-cases-stay-flat-fifth-day-row-90-629-expert-says-Omicron-peaked.html
https://www.edp24.co.uk/news/health/omicron-covid-cases-peak-alastair-grant-uea-norfolk-8578854
Prof Pagel; only in the most recent week has Omicron been dominant and it takes about 10-14 days from infection to needing hospital.
We have the benefit of sitting back and observing what actually happens.
I am not sure the old rules apply now because there are so many in the UK who are either vaccinated or have previously had Covid, so there is a lot of base immunity that at least reduces the severity of symptoms.
Also, there are very effective anti-viral drugs now that often prevent Covid from becoming serious.
So, the impact may be a lot less severe than some are predicting.
https://www.rnz.co.nz/news/national/458424/omicron-spreads-faster-than-delta-but-definitive-data-on-severity-is-a-waiting-game-researcher
And, whatever short term evidence we get for acute infections, the rate at which omicron causes long covid (and the severity of that) won't be known for months, or longer. Think that one through. If we relaxed and let omicron spread then it turns out that 40% of NZers get long term symptoms, and 20% of those can no longer work.
Yes, I have seen that. That study is based on a very small subset of data, so can hardly be seen as definitive. Neither has it been peer-reviewed.
https://www.nbcchicago.com/news/local/omicron-symptoms-what-we-know-about-the-severity-of-the-new-variant/2710433/
From the article:
The data included 24 hospitalizations of patients suspected of having the omicron variant, with researchers saying "hospitalisation data remains very limited at this time." The study is yet to be peer-reviewed.
On the face of it, there is also a huge data skew between the group testing positive for Omicron vs those that tested positive for other variations. Given that on 24 out of the approx 11000 were in hospital suggests the hospitalisation rate is very low, at least thus far.
The other thing is, that even if Omicron is just as severe, the environment it replicates in is very different. There is a lot of vaccine and natural immunity to Covid generally, plus we have very effective anti-virals now. So, even if it is just as severe as other mutations, it doesn’t mean it will cause anything like as much harm.
Further to that, there are various statistical transformations that can be used to compare groups where there is large skews such as above. However, these sort of techniques can be a bit artificial in their outcomes.
If it were me I would have randomly selected 11000 cases from the 200000 comparator group to compare against the Omicron group.
This then would be comparing apples with apples.
You're missing the point. Which is that, we cannot know yet. It will take weeks to know about the acute effects, and months or longer to know about the chronic effects. Anything push at the moment to basing pandemic response on omicron reckons is wishful thinking and dangerous.
I absolutely agree with you on that point. If you read back over my previous posts, you will see that I have said similar, and that I agree with the government's decision to keep the border closed a bit longer.
I am just looking at the situation more positively, with the hope that Omicron turns out to be much less harmful than what people think. I am just putting forward the case that there is evidence that Omicron may turn out to be not such a worry.
That is something we would all like to see, surely.
NHS England has recorded almost a doubling of daily hospitalisations in London in 2 weeks.
The government must hold the line here especially against short term thinking.
Kia Kaha Weka.
cheers, pukahu.
Here is a very good article from England:
https://news.sky.com/story/omicron-what-do-covid-hospitalisation-figures-in-london-tell-us-about-how-severe-the-new-variant-is-12501451
Look at the second graph down. That is a chart showing a rolling 7 day average of Covid cases compared to a seven day lag of hospitalisation rates.
Notice how good the match is from April 2020.
The hospitalisation rates are increasing slightly at the moment. But nothing like the rise in Covid cases.
The whole article is very informative on this issue.