 Covid-19 lessons from a plagued flight
Covid-19 lessons from a plagued flight
Written By:
- Date published:
10:43 pm, January 11th, 2021 - 22 comments
Categories: covid-19 -
Tags: air travel crisis, bubble, genomic detectives
In September there was a 18 hour flight Dubai that ended in Auckland. A relatively close group on that plane showed infection after arrival, and a genetically similar version. The evidence of in-flight infection is very strong and points to the on-going issues with shipping virus hosts around the world. This has some pretty strong implications for long-haul flights in particular. But also to the risks of having travel ‘bubbles’ without enforced quarantine.
On September 29, 2020, flight EK448, which originated in Dubai, United Arab Emirates, with a stop in Kuala Lumpur, Malaysia, landed in Auckland, New Zealand. During the required 14-day MIQ period, 7 passengers who had traveled on the flight received positive SARS-CoV-2 test results. The 7 passengers had begun their journeys from 5 different countries before a layover in Dubai; predeparture SARS-CoV-2 test results were negative for 5 (Figure 1). These 7 passengers had been seated within 4 rows of each other during the ≈18-hour flight from Dubai to Auckland. Because recent studies have reported conflicting findings of the risks associated with in-flight transmission (2–4), we undertook a comprehensive investigation to determine the potential source of infection of these travelers.
CDC – Emerging Infectious Diseases: “Genomic Evidence of In-Flight Transmission of SARS-CoV-2 Despite Predeparture Testing“
There is a lot of information in the early release article about the process of the travel of the people infected and of the flight. Reading through it, there are some obvious possible holes like mask and glove wearing on the flight. The 2 hour refuelling stop over in Kuala Lumpur had no passengers on or off. However it did have a auxilary power unit off for 30 minutes during that time, and therefore no environmental control during that period – a possible contributing factor.
The abstract states (my italics) in its conclusion..
Among 86 passengers on a flight from Dubai, United Arab Emirates, that arrived in New Zealand on September 29, test results were positive for 7 persons in MIQ. These passengers originated from 5 different countries before a layover in Dubai; 5 had negative predeparture SARS-CoV-2 test results. To assess possible points of infection, we analyzed information about their journeys, disease progression, and virus genomic data. All 7 SARS-CoV-2 genomes were genetically identical, except for a single mutation in 1 sample. Despite predeparture testing, multiple instances of in-flight SARS-CoV-2 transmission are likely.
CDC – Emerging Infectious Diseases: “Genomic Evidence of In-Flight Transmission of SARS-CoV-2 Despite Predeparture Testing“
For me the figures in the article are the most explanatory. So I’m going to put them up.

Figure 1. Countries of travel origins for 7 passengers who tested positive for severe acute respiratory syndrome coronavirus 2 infection after traveling on the same flight (EK448) from Dubai, United Arab Emirates, to Auckland, New Zealand, with a refueling stop in Kuala Lumpur, Malaysia, on September 29, 2020. Asterisks indicate where 6 other genetically identical genomes have been reported
The most notable part of the image is the diversity of locations that the infected passengers came from. The probability of having the same covid-19 genome is very low. But the likely incubation times and times of the tests is even more interesting.

Figure 2. Timeline of likely incubation and infectious periods, indicating testing dates, for 7 passengers who tested positive for severe acute respiratory syndrome coronavirus 2 infection after traveling on the same flight (EK448) from Dubai, United Arab Emirates, to Auckland, New Zealand, with a refueling stop in Kuala Lumpur, Malaysia, on September 29, 2020.
As is the positioning of these seven passengers in a spaced out flight. Not to mention the locations of the passengers who didn’t get positive tests. Look at seats 24E, 24G and 28D and 26C – obviously either very lucky or had very nasty immune systems.
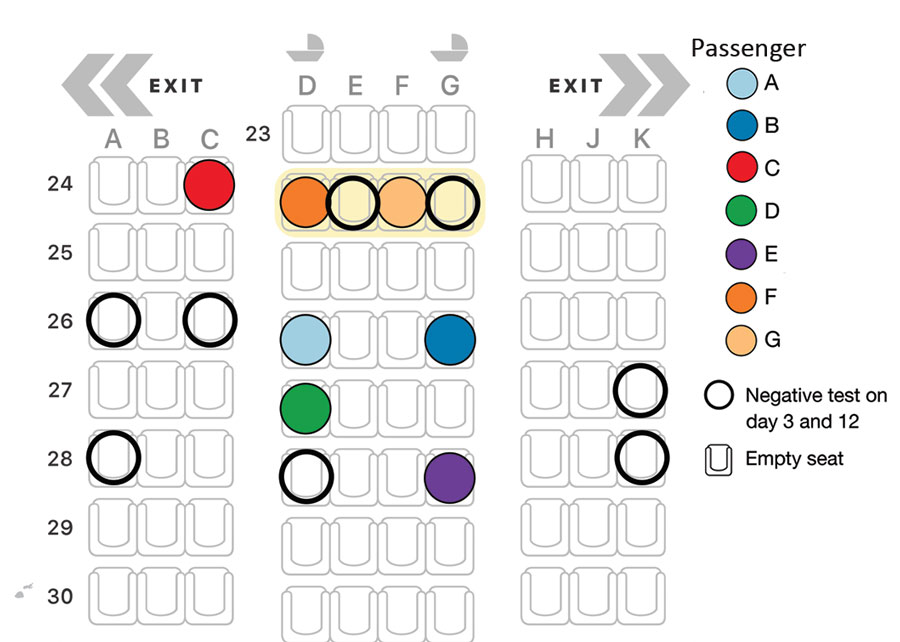
Figure 3. Seating arrangement (Boeing 777–300ER) for 7 passengers who tested positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection on flight EK448 from Dubai, United Arab Emirates, to Auckland, New Zealand, with a refueling stop in Kuala Lumpur, Malaysia, on September 29, 2020. Passengers F and G interchanged seats within row 24. Open circles represent nearby passengers who were negative for SARS-CoV-2 on days 3 and 12 while in managed isolation and quarantine. All other seats shown remained empty.
Figure 4 is the analysis genomic family. It is a extremely close match, especially from a group from such diverse locations.
The final figure is quite interesting as it uses the anticipated times and seating to try to look at possible transmission paths. Look at it in conjunction with figures 2 and 3.
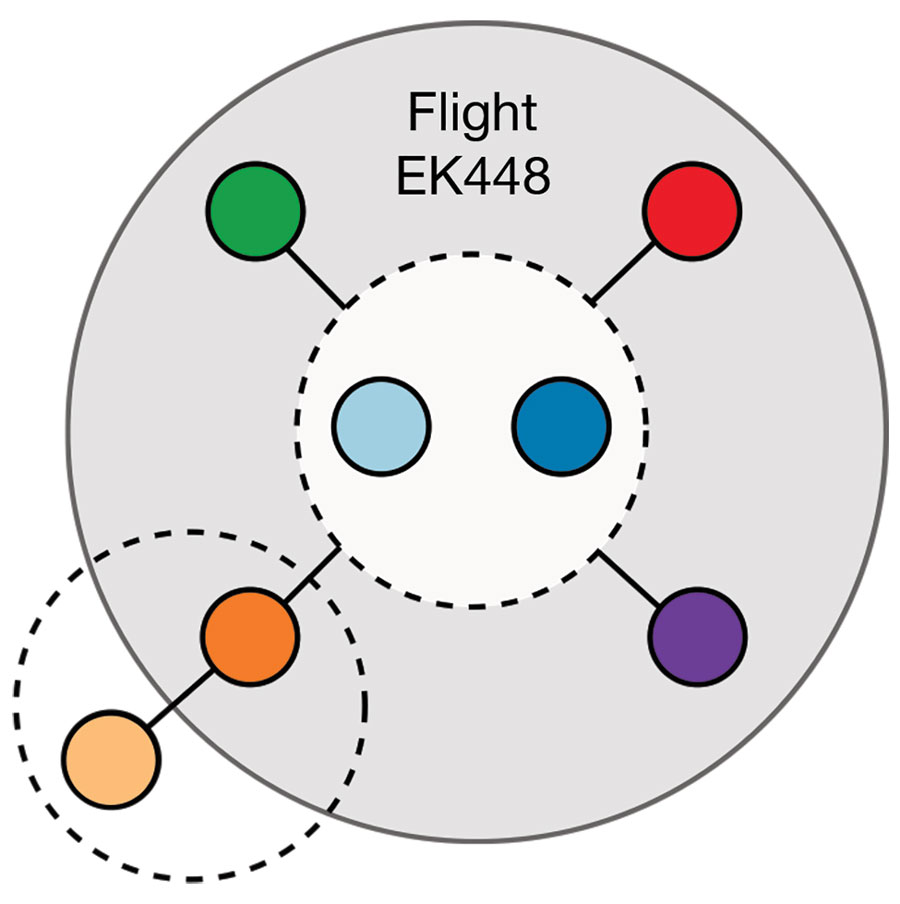
Figure 5. Network of likely severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) transmission among 7 passengers who traveled on flight EK448 (Boeing 777–300ER) from Dubai, United Arab Emirates, to Auckland, New Zealand, with a refueling stop in Kuala Lumpur, Malaysia, on September 29, 2020. The gray shaded area illustrates likely in-flight virus transmission. Dashed circles represent likely virus transmission between travel companions.
What is notable from this is that it shows the several notable characteristics of this disease.
It is infectious, but nothing like the same order as influenza. In an 18 hour flight even with precautions, a more virulent infection would have probably infected more people in the immediate vicinity. In particular the pattern in row 24 with the two people not getting a positive result is pretty abnormal.
The preflight checks were essentially useless and probably gave a false sense of security for both crew and passengers. That is my primary dislike for such tests – people can and will get tests both before getting infected and also return negative results if they have just been infected. On a long haul flight, they will infect others. The time taken before the disease is detectable by symptoms or test compared to the time to become infections is such that it is really hard to detect for flight onboarding.
That is the primary reason you won’t get my 61yo body in a long haul aircraft anytime soon. They are the ideal infection canisters for covid-19, if not on the way out, then on the way home again.
The same considerations apply for local no-quarantine travel bubbles where there are repeated unexplained community outbreaks – such as we have been seeing repeatably in Australia. Someone who is infected can be happily walking around after testing negative, and without a strong receiving quarantine infect others in-flight or after arrival.
Bearing in mind the financial and economic costs of suppression in the order of what we or the Australians have done to date, and the much smaller costs of strong border controls – this is a economic no-brainer for the country as a whole.
Incidentally, for an individual to have a vaccines don’t make as much of a difference as you’d expect. Ignoring the time to them becoming effective (a not inconsiderable consideration). Then even when and individual is fully vaccinated they are better at stopping the infection from spreading inside the individual than they are in stopping others being infected. The reason is that the bodies defences have noticeable delays at suppression after infection, and many if not most vaccinated people will be infectious.
Personally I don’t want to fly until I’ve had a chance to see what happens in the real world with vaccines in my age group. I sure as hell don’t want vaccinated Aussie tourists or returning kiwis here without quarantine until both countries have a sufficient induced population immunity to reduce the risks to an acceptable level. Certainly not to benefit airlines. tourism operators, and universities. After all they’re not paying me anything to negate the risks I would carry for them.
Just as importantly, this demonstrates the diagnostic utility of getting genomic analysis correlated with travel patterns.
There is more analysis in New York Times “One 18-Hour Flight, Four Coronavirus Infections“. However the title seems like a somewhat optimistic reading of the evidence.
22 comments on “Covid-19 lessons from a plagued flight ”
- Comments are now closed
- Comments are now closed
Recent Comments
- Bernard’s Saturday Soliloquy for the week to July 27
 Photo: Lynn Grieveson / The KākāTL;DR: My top six things to note around housing, climate and poverty in Aotearoa’s political economy in the week to July 27 were:1. The Minister for Ford Rangers strikes againTransport Minister Simeon Brown was again the busiest of the Cabinet ministers this week, announcing an ...43 seconds ago
Photo: Lynn Grieveson / The KākāTL;DR: My top six things to note around housing, climate and poverty in Aotearoa’s political economy in the week to July 27 were:1. The Minister for Ford Rangers strikes againTransport Minister Simeon Brown was again the busiest of the Cabinet ministers this week, announcing an ...43 seconds ago - Ticket To Anywhere
 You got a fast carAnd I want a ticket to anywhereMaybe we make a dealMaybe together we can get somewhereAny place is betterYesterday’s newsletter, Trust In Me, on the report of abuse in state care, and by religious organisations, between 1950 and 2019, coupled with the hypocrisy of Christopher Luxon ...43 mins ago
You got a fast carAnd I want a ticket to anywhereMaybe we make a dealMaybe together we can get somewhereAny place is betterYesterday’s newsletter, Trust In Me, on the report of abuse in state care, and by religious organisations, between 1950 and 2019, coupled with the hypocrisy of Christopher Luxon ...43 mins ago - Stories of varying weight
 5 hours ago
5 hours ago - Balancing External Security and the Economy
 New Zealand is again having to reconcile conflicting pressures from its military and its trade interests. Should we join Pillar Two of AUKUS and risk compromising our markets in China? For a century after New Zealand was founded in 1840, its external security arrangements and external economics arrangements were aligned. ...18 hours ago
New Zealand is again having to reconcile conflicting pressures from its military and its trade interests. Should we join Pillar Two of AUKUS and risk compromising our markets in China? For a century after New Zealand was founded in 1840, its external security arrangements and external economics arrangements were aligned. ...18 hours ago - Weekly Climate Wrap: The unravelling of the offsets
23 hours ago
- What makes us tick
 This morning the sky was bright.The birds, in their usual joyous bliss. Nature doesn’t seem to feel the heat of what might angst humans.Their calls are clear and beautiful.Just some random thoughts:MāoriPaul Goldsmith has announced his government will roll back the judiciary’s rulings on Māori Customary Marine Title, which recognises ...24 hours ago
This morning the sky was bright.The birds, in their usual joyous bliss. Nature doesn’t seem to feel the heat of what might angst humans.Their calls are clear and beautiful.Just some random thoughts:MāoriPaul Goldsmith has announced his government will roll back the judiciary’s rulings on Māori Customary Marine Title, which recognises ...24 hours ago - Foreshore and seabed 2.0
 In 2003, the Court of Appeal delivered its decision in Ngati Apa v Attorney-General, ruling that Māori customary title over the foreshore and seabed had not been universally extinguished, and that the Māori Land Court could determine claims and confirm title if the facts supported it. This kicked off the ...1 day ago
In 2003, the Court of Appeal delivered its decision in Ngati Apa v Attorney-General, ruling that Māori customary title over the foreshore and seabed had not been universally extinguished, and that the Māori Land Court could determine claims and confirm title if the facts supported it. This kicked off the ...1 day ago - Gordon Campbell on the Royal Commission report into abuse in care
 Earlier this week at Parliament, Labour leader Chris Hipkins was applauded for saying that the response to the final report of the Royal Commission of Inquiry into Abuse in Care had to be “bigger than politics.” True, but the fine words, apologies and “we hear you” messages will soon ring ...1 day ago
Earlier this week at Parliament, Labour leader Chris Hipkins was applauded for saying that the response to the final report of the Royal Commission of Inquiry into Abuse in Care had to be “bigger than politics.” True, but the fine words, apologies and “we hear you” messages will soon ring ...1 day ago - The Kākā’s Pick 'n' Mix for Friday, July 26
 TL;DR: In news breaking this morning:The Ministry of Education is cutting $2 billion from its school building programme so the National-ACT-NZ First Coalition Government has enough money to deliver tax cuts; The Government has quietly lowered its child poverty reduction targets to make them easier to achieve;Te Whatu Ora-Health NZ’s ...1 day ago
TL;DR: In news breaking this morning:The Ministry of Education is cutting $2 billion from its school building programme so the National-ACT-NZ First Coalition Government has enough money to deliver tax cuts; The Government has quietly lowered its child poverty reduction targets to make them easier to achieve;Te Whatu Ora-Health NZ’s ...1 day ago - Weekly Roundup 26-July-2024
 Kia ora. These are some stories that caught our eye this week – as always, feel free to share yours in the comments. Our header image this week (via Eke Panuku) shows the planned upgrade for the Karanga Plaza Tidal Swimming Steps. The week in Greater Auckland On ...1 day ago
Kia ora. These are some stories that caught our eye this week – as always, feel free to share yours in the comments. Our header image this week (via Eke Panuku) shows the planned upgrade for the Karanga Plaza Tidal Swimming Steps. The week in Greater Auckland On ...1 day ago - God what a relief
 1 day ago
1 day ago - Trust In Me
 Trust in me in all you doHave the faith I have in youLove will see us through, if only you trust in meWhy don't you, you trust me?In a week that saw the release of the 3,000 page Abuse in Care report Christopher Luxon was being asked about Boot Camps. ...1 day ago
Trust in me in all you doHave the faith I have in youLove will see us through, if only you trust in meWhy don't you, you trust me?In a week that saw the release of the 3,000 page Abuse in Care report Christopher Luxon was being asked about Boot Camps. ...1 day ago - The Hoon around the week to July 26
TL;DR: The podcast above of the weekly ‘hoon’ webinar for paying subscribers last night features co-hosts and talking about the Royal Commission Inquiry into Abuse in Care report released this week, and with:The Kākā’s climate correspondent on a UN push to not recognise carbon offset markets and ...1 day ago
- The Kākā’s Journal of Record for Friday, July 26
 TL;DR: As of 6:00 am on Friday, July 26, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:Transport: Simeon Brown announced $802.9 million in funding for 18 new trains on the Wairarapa and Manawatū rail lines, which ...1 day ago
TL;DR: As of 6:00 am on Friday, July 26, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:Transport: Simeon Brown announced $802.9 million in funding for 18 new trains on the Wairarapa and Manawatū rail lines, which ...1 day ago - Radical law changes needed to build road
The northern expressway extension from Warkworth to Whangarei is likely to require radical changes to legislation if it is going to be built within the foreseeable future. The Government’s powers to purchase land, the planning process and current restrictions on road tolling are all going to need to be changed ...1 day ago
- Skeptical Science New Research for Week #30 2024
 Open access notables Could an extremely cold central European winter such as 1963 happen again despite climate change?, Sippel et al., Weather and Climate Dynamics: Here, we first show based on multiple attribution methods that a winter of similar circulation conditions to 1963 would still lead to an extreme seasonal ...2 days ago
Open access notables Could an extremely cold central European winter such as 1963 happen again despite climate change?, Sippel et al., Weather and Climate Dynamics: Here, we first show based on multiple attribution methods that a winter of similar circulation conditions to 1963 would still lead to an extreme seasonal ...2 days ago - First they came for the Māori
 2 days ago
2 days ago - Join us for the weekly Hoon on YouTube Live
 Photo by Joshua J. Cotten on UnsplashWe’re back again after our mid-winter break. We’re still with the ‘new’ day of the week (Thursday rather than Friday) when we have our ‘hoon’ webinar with paying subscribers to The Kākā for an hour at 5 pm.Jump on this link on YouTube Livestream ...2 days ago
Photo by Joshua J. Cotten on UnsplashWe’re back again after our mid-winter break. We’re still with the ‘new’ day of the week (Thursday rather than Friday) when we have our ‘hoon’ webinar with paying subscribers to The Kākā for an hour at 5 pm.Jump on this link on YouTube Livestream ...2 days ago - Will the real PM Luxon please stand up?
 2 days ago
2 days ago - Will debt reduction trump abuse in care redress?
 Luxon speaks in Parliament yesterday about the Abuse in Care report. Photo: Hagen Hopkins/Getty ImagesTL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy today are:PM Christopher Luxon said yesterday in tabling the Abuse in Care report in Parliament he wanted to ‘do the ...2 days ago
Luxon speaks in Parliament yesterday about the Abuse in Care report. Photo: Hagen Hopkins/Getty ImagesTL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy today are:PM Christopher Luxon said yesterday in tabling the Abuse in Care report in Parliament he wanted to ‘do the ...2 days ago - Olywhites and Time Bandits
 About a decade ago I worked with a bloke called Steve. He was the grizzled veteran coder, a few years older than me, who knew where the bodies were buried - code wise. Despite his best efforts to be approachable and friendly he could be kind of gruff, through to ...2 days ago
About a decade ago I worked with a bloke called Steve. He was the grizzled veteran coder, a few years older than me, who knew where the bodies were buried - code wise. Despite his best efforts to be approachable and friendly he could be kind of gruff, through to ...2 days ago - Why were the 1930s so hot in North America?
This is a re-post from Yale Climate Connections by Jeff Masters and Bob Henson Those who’ve trawled social media during heat waves have likely encountered a tidbit frequently used to brush aside human-caused climate change: Many U.S. states and cities had their single hottest temperature on record during the 1930s, setting incredible heat marks ...2 days ago
- Throwback Thursday – Thinking about Expressways
Some of the recent announcements from the government have reminded us of posts we’ve written in the past. Here’s one from early 2020. There were plenty of reactions to the government’s infrastructure announcement a few weeks ago which saw them fund a bunch of big roading projects. One of ...2 days ago
- The Kākā’s Pick 'n' Mix for Thursday, July 25
 TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 7:00 am on Thursday, July 25 are:News: Why Electric Kiwi is closing to new customers - and why it matters RNZ’s Susan EdmundsScoop: Government drops ...2 days ago
TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 7:00 am on Thursday, July 25 are:News: Why Electric Kiwi is closing to new customers - and why it matters RNZ’s Susan EdmundsScoop: Government drops ...2 days ago - The Possum: Demon or Friend?
 Hi,I felt a small wet tongue snaking through one of the holes in my Crocs. It explored my big toe, darting down one side, then the other. “He’s looking for some toe cheese,” said the woman next to me, words that still haunt me to this day.Growing up in New ...2 days ago
Hi,I felt a small wet tongue snaking through one of the holes in my Crocs. It explored my big toe, darting down one side, then the other. “He’s looking for some toe cheese,” said the woman next to me, words that still haunt me to this day.Growing up in New ...2 days ago - Not a story
 Yesterday I happily quoted the Prime Minister without fact-checking him and sure enough, it turns out his numbers were all to hell. It’s not four kg of Royal Commission report, it’s fourteen.My friend and one-time colleague-in-comms Hazel Phillips gently alerted me to my error almost as soon as I’d hit ...2 days ago
Yesterday I happily quoted the Prime Minister without fact-checking him and sure enough, it turns out his numbers were all to hell. It’s not four kg of Royal Commission report, it’s fourteen.My friend and one-time colleague-in-comms Hazel Phillips gently alerted me to my error almost as soon as I’d hit ...2 days ago - The Kākā’s Journal of Record for Thursday, July 25
 TL;DR: As of 6:00 am on Thursday, July 25, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day were:The Abuse in Care Royal Commission of Inquiry published its final report yesterday.PM Christopher Luxon and The Minister responsible for ...2 days ago
TL;DR: As of 6:00 am on Thursday, July 25, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day were:The Abuse in Care Royal Commission of Inquiry published its final report yesterday.PM Christopher Luxon and The Minister responsible for ...2 days ago - A tougher line on “proactive release”?
The Official Information Act has always been a battle between requesters seeking information, and governments seeking to control it. Information is power, so Ministers and government agencies want to manage what is released and when, for their own convenience, and legality and democracy be damned. Their most recent tactic for ...3 days ago
- 'Let's build a motorway costing $100 million per km, before emissions costs'
 TL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy today are:Transport and Energy Minister Simeon Brown is accelerating plans to spend at least $10 billion through Public Private Partnerships (PPPs) to extend State Highway One as a four-lane ‘Expressway’ from Warkworth to Whangarei ...3 days ago
TL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy today are:Transport and Energy Minister Simeon Brown is accelerating plans to spend at least $10 billion through Public Private Partnerships (PPPs) to extend State Highway One as a four-lane ‘Expressway’ from Warkworth to Whangarei ...3 days ago - Lester's Prescription – Positive Bleeding.
 I live my life (woo-ooh-ooh)With no control in my destinyYea-yeah, yea-yeah (woo-ooh-ooh)I can bleed when I want to bleedSo come on, come on (woo-ooh-ooh)You can bleed when you want to bleedYea-yeah, come on (woo-ooh-ooh)Everybody bleed when they want to bleedCome on and bleedGovernments face tough challenges. Selling unpopular decisions to ...3 days ago
I live my life (woo-ooh-ooh)With no control in my destinyYea-yeah, yea-yeah (woo-ooh-ooh)I can bleed when I want to bleedSo come on, come on (woo-ooh-ooh)You can bleed when you want to bleedYea-yeah, come on (woo-ooh-ooh)Everybody bleed when they want to bleedCome on and bleedGovernments face tough challenges. Selling unpopular decisions to ...3 days ago - Casey Costello gaslights Labour in the House
Please note:To skip directly to the- parliamentary footage in the video, scroll to 1:21 To skip to audio please click on the headphone icon on the left hand side of the screenThis video / audio section is under development. ...3 days ago
- Why is the Texas grid in such bad shape?
This is a re-post from the Climate Brink by Andrew Dessler Headline from 2021 The Texas grid, run by ERCOT, has had a rough few years. In 2021, winter storm Uri blacked out much of the state for several days. About a week ago, Hurricane Beryl knocked out ...3 days ago
- Gordon Campbell on a textbook case of spending waste by the Luxon government
Given the crackdown on wasteful government spending, it behooves me to point to a high profile example of spending by the Luxon government that looks like a big, fat waste of time and money. I’m talking about the deployment of NZDF personnel to support the US-led coalition in the Red ...3 days ago
- The Kākā’s Pick 'n' Mix for Wednesday, July 24
 TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 7:40 am on Wednesday, July 24 are:Deep Dive: Chipping away at the housing crisis, including my comments RNZ/Newsroom’s The DetailNews: Government softens on asset sales, ...3 days ago
TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 7:40 am on Wednesday, July 24 are:Deep Dive: Chipping away at the housing crisis, including my comments RNZ/Newsroom’s The DetailNews: Government softens on asset sales, ...3 days ago - LXR Takaanini
As I reported about the city centre, Auckland’s rail network is also going through a difficult and disruptive period which is rapidly approaching a culmination, this will result in a significant upgrade to the whole network. Hallelujah. Also like the city centre this is an upgrade predicated on the City ...3 days ago
- Four kilograms of pain
 Today, a 4 kilogram report will be delivered to Parliament. We know this is what the report of the Royal Commission of Inquiry into Abuse in State and Faith-based Care weighs, because our Prime Minister told us so.Some reporter had blindsided him by asking a question about something done by ...3 days ago
Today, a 4 kilogram report will be delivered to Parliament. We know this is what the report of the Royal Commission of Inquiry into Abuse in State and Faith-based Care weighs, because our Prime Minister told us so.Some reporter had blindsided him by asking a question about something done by ...3 days ago - The Kākā’s Journal of Record for Wednesday, July 24
 TL;DR: As of 7:00 am on Wednesday, July 24, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:Beehive: Transport Minister Simeon Brown announced plans to use PPPs to fund, build and run a four-lane expressway between Auckland ...3 days ago
TL;DR: As of 7:00 am on Wednesday, July 24, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:Beehive: Transport Minister Simeon Brown announced plans to use PPPs to fund, build and run a four-lane expressway between Auckland ...3 days ago - Luxon gets caught out
NewstalkZB host Mike Hosking, who can usually be relied on to give Prime Minister Christopher Luxon an easy run, did not do so yesterday when he interviewed him about the HealthNZ deficit. Luxon is trying to use a deficit reported last year by HealthNZ as yet another example of the ...3 days ago
- A worrying sign
Back in January a StatsNZ employee gave a speech at Rātana on behalf of tangata whenua in which he insulted and criticised the government. The speech clearly violated the principle of a neutral public service, and StatsNZ started an investigation. Part of that was getting an external consultant to examine ...4 days ago
- Are we fine with 47.9% home-ownership by 2048?
 Renting for life: Shared ownership initiatives are unlikely to slow the slide in home ownership by much. Photo: Lynn Grieveson / The KākāTL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy today are:A Deloitte report for Westpac has projected Aotearoa’s home-ownership rate will ...4 days ago
Renting for life: Shared ownership initiatives are unlikely to slow the slide in home ownership by much. Photo: Lynn Grieveson / The KākāTL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy today are:A Deloitte report for Westpac has projected Aotearoa’s home-ownership rate will ...4 days ago - Let's Win This
 You're broken down and tiredOf living life on a merry go roundAnd you can't find the fighterBut I see it in you so we gonna walk it outAnd move mountainsWe gonna walk it outAnd move mountainsAnd I'll rise upI'll rise like the dayI'll rise upI'll rise unafraidI'll rise upAnd I'll ...4 days ago
You're broken down and tiredOf living life on a merry go roundAnd you can't find the fighterBut I see it in you so we gonna walk it outAnd move mountainsWe gonna walk it outAnd move mountainsAnd I'll rise upI'll rise like the dayI'll rise upI'll rise unafraidI'll rise upAnd I'll ...4 days ago - Waimahara: The Singing Spirit of Water
There’s been a change in Myers Park. Down the steps from St. Kevin’s Arcade, past the grassy slopes, the children’s playground, the benches and that goat statue, there has been a transformation. The underpass for Mayoral Drive has gone from a barren, grey, concrete tunnel, to a place that thrums ...4 days ago
- A major milestone: Global climate pollution may have just peaked
This is a re-post from Yale Climate Connections Global society may have finally slammed on the brakes for climate-warming pollution released by human fossil fuel combustion. According to the Carbon Monitor Project, the total global climate pollution released between February and May 2024 declined slightly from the amount released during the same ...4 days ago
- The Kākā’s Pick 'n' Mix for Tuesday, July 23
 TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 7:00 am on Tuesday, July 23 are:Deep Dive: Penlink: where tolling rhetoric meets reality BusinessDesk-$$$’s Oliver LewisScoop: Te Pūkenga plans for regional polytechs leak out ...4 days ago
TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 7:00 am on Tuesday, July 23 are:Deep Dive: Penlink: where tolling rhetoric meets reality BusinessDesk-$$$’s Oliver LewisScoop: Te Pūkenga plans for regional polytechs leak out ...4 days ago - The Kākā’s Journal of Record for Tuesday, July 23
 TL;DR: As of 6:00 am on Tuesday, July 23, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:Health: Shane Reti announced the Board of Te Whatu Ora- Health New Zealand was being replaced with Commissioner Lester Levy ...4 days ago
TL;DR: As of 6:00 am on Tuesday, July 23, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:Health: Shane Reti announced the Board of Te Whatu Ora- Health New Zealand was being replaced with Commissioner Lester Levy ...4 days ago - HealthNZ and Luxon at cross purposes over budget blowout
Health NZ warned the Government at the end of March that it was running over Budget. But the reasons it gave were very different to those offered by the Prime Minister yesterday. Prime Minister Christopher Luxon blamed the “botched merger” of the 20 District Health Boards (DHBs) to create Health ...4 days ago
- 2500-3000 more healthcare staff expected to be fired, as Shane Reti blames Labour for a budget defic...
 Long ReadKey Summary: Although National increased the health budget by $1.4 billion in May, they used an old funding model to project health system costs, and never bothered to update their pre-election numbers. They were told during the Health Select Committees earlier in the year their budget amount was deficient, ...4 days ago
Long ReadKey Summary: Although National increased the health budget by $1.4 billion in May, they used an old funding model to project health system costs, and never bothered to update their pre-election numbers. They were told during the Health Select Committees earlier in the year their budget amount was deficient, ...4 days ago - Might Kamala Harris be about to get a 'stardust' moment like Jacinda Ardern?
 As a momentous, historic weekend in US politics unfolded, analysts and commentators grasped for precedents and comparisons to help explain the significance and power of the choice Joe Biden had made. The 46th president had swept the Democratic party’s primaries but just over 100 days from the election had chosen ...5 days ago
As a momentous, historic weekend in US politics unfolded, analysts and commentators grasped for precedents and comparisons to help explain the significance and power of the choice Joe Biden had made. The 46th president had swept the Democratic party’s primaries but just over 100 days from the election had chosen ...5 days ago - Solutions Interview: Steven Hail on MMT & ecological economics
TL;DR: I’m casting around for new ideas and ways of thinking about Aotearoa’s political economy to find a few solutions to our cascading and self-reinforcing housing, poverty and climate crises.Associate Professor runs an online masters degree in the economics of sustainability at Torrens University in Australia and is organising ...5 days ago
- Reported back
The Finance and Expenditure Committee has reported back on National's Local Government (Water Services Preliminary Arrangements) Bill. The bill sets up water for privatisation, and was introduced under urgency, then rammed through select committee with no time even for local councils to make a proper submission. Naturally, national's select committee ...5 days ago
- Vandrad the Viking, Christopher Coombes, and Literary Archaeology
 Some years ago, I bought a book at Dunedin’s Regent Booksale for $1.50. As one does. Vandrad the Viking (1898), by J. Storer Clouston, is an obscure book these days – I cannot find a proper online review – but soon it was sitting on my shelf, gathering dust alongside ...5 days ago
Some years ago, I bought a book at Dunedin’s Regent Booksale for $1.50. As one does. Vandrad the Viking (1898), by J. Storer Clouston, is an obscure book these days – I cannot find a proper online review – but soon it was sitting on my shelf, gathering dust alongside ...5 days ago - Gordon Campbell On The Biden Withdrawal
History is not on the side of the centre-left, when Democratic presidents fall behind in the polls and choose not to run for re-election. On both previous occasions in the past 75 years (Harry Truman in 1952, Lyndon Johnson in 1968) the Democrats proceeded to then lose the White House ...5 days ago
- Joe Biden's withdrawal puts the spotlight back on Kamala and the USA's complicated relatio...
 This is a free articleCoverageThis morning, US President Joe Biden announced his withdrawal from the Presidential race. And that is genuinely newsworthy. Thanks for your service, President Biden, and all the best to you and yours.However, the media in New Zealand, particularly the 1News nightly bulletin, has been breathlessly covering ...5 days ago
This is a free articleCoverageThis morning, US President Joe Biden announced his withdrawal from the Presidential race. And that is genuinely newsworthy. Thanks for your service, President Biden, and all the best to you and yours.However, the media in New Zealand, particularly the 1News nightly bulletin, has been breathlessly covering ...5 days ago - Why we have to challenge our national fiscal assumptions
 A homeless person’s camp beside a blocked-off slipped damage walkway in Freeman’s Bay: we are chasing our tail on our worsening and inter-related housing, poverty and climate crises. Photo: Photo: Lynn Grieveson / The KākāTL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy ...5 days ago
A homeless person’s camp beside a blocked-off slipped damage walkway in Freeman’s Bay: we are chasing our tail on our worsening and inter-related housing, poverty and climate crises. Photo: Photo: Lynn Grieveson / The KākāTL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy ...5 days ago - Existential Crisis and Damaged Brains
 What has happened to it all?Crazy, some'd sayWhere is the life that I recognise?(Gone away)But I won't cry for yesterdayThere's an ordinary worldSomehow I have to findAnd as I try to make my wayTo the ordinary worldYesterday morning began as many others - what to write about today? I began ...5 days ago
What has happened to it all?Crazy, some'd sayWhere is the life that I recognise?(Gone away)But I won't cry for yesterdayThere's an ordinary worldSomehow I have to findAnd as I try to make my wayTo the ordinary worldYesterday morning began as many others - what to write about today? I began ...5 days ago - A speed limit is not a target, and yet…
This is a guest post from longtime supporter Mr Plod, whose previous contributions include a proposal that Hamilton become New Zealand’s capital city, and that we should switch which side of the road we drive on. A recent Newsroom article, “Back to school for the Govt’s new speed limit policy“, ...5 days ago
- The Kākā’s Pick 'n' Mix for Monday, July 22
 TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 7:00 am on Monday, July 22 are:Today’s Must Read: Father and son live in a tent, and have done for four years, in a million ...5 days ago
TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 7:00 am on Monday, July 22 are:Today’s Must Read: Father and son live in a tent, and have done for four years, in a million ...5 days ago - The Kākā’s Journal of Record for Monday, July 22
 TL;DR: As of 7:00 am on Monday, July 22, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:US President Joe Biden announced via X this morning he would not stand for a second term.Multinational professional services firm ...5 days ago
TL;DR: As of 7:00 am on Monday, July 22, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:US President Joe Biden announced via X this morning he would not stand for a second term.Multinational professional services firm ...5 days ago - 2024 SkS Weekly Climate Change & Global Warming News Roundup #29
A listing of 32 news and opinion articles we found interesting and shared on social media during the past week: Sun, July 14, 2024 thru Sat, July 20, 2024. Story of the week As reflected by preponderance of coverage, our Story of the Week is Project 2025. Until now traveling ...6 days ago
- I'd like to share what I did this weekend
 6 days ago
6 days ago - For the children – Why mere sentiment can be a misleading force in our lives, and lead to unex...
 National: The Party of ‘Law and Order’ IntroductionThis weekend, the Government formally kicked off one of their flagship policy programs: a military style boot camp that New Zealand has experimented with over the past 50 years. Cartoon credit: Guy BodyIt’s very popular with the National Party’s Law and Order image, ...6 days ago
National: The Party of ‘Law and Order’ IntroductionThis weekend, the Government formally kicked off one of their flagship policy programs: a military style boot camp that New Zealand has experimented with over the past 50 years. Cartoon credit: Guy BodyIt’s very popular with the National Party’s Law and Order image, ...6 days ago - A friend in uncertain times
 Day one of the solo leg of my long journey home begins with my favourite sound: footfalls in an empty street. 5.00 am and it’s already light and already too warm, almost.If I can make the train that leaves Budapest later this hour I could be in Belgrade by nightfall; ...6 days ago
Day one of the solo leg of my long journey home begins with my favourite sound: footfalls in an empty street. 5.00 am and it’s already light and already too warm, almost.If I can make the train that leaves Budapest later this hour I could be in Belgrade by nightfall; ...6 days ago - The Chaotic World of Male Diet Influencers
 Hi,We’ll get to the horrific world of male diet influencers (AKA Beefy Boys) shortly, but first you will be glad to know that since I sent out the Webworm explaining why the assassination attempt on Donald Trump was not a false flag operation, I’ve heard from a load of people ...6 days ago
Hi,We’ll get to the horrific world of male diet influencers (AKA Beefy Boys) shortly, but first you will be glad to know that since I sent out the Webworm explaining why the assassination attempt on Donald Trump was not a false flag operation, I’ve heard from a load of people ...6 days ago - It's Starting To Look A Lot Like… Y2K
 Do you remember Y2K, the threat that hung over humanity in the closing days of the twentieth century? Horror scenarios of planes falling from the sky, electronic payments failing and ATMs refusing to dispense cash. As for your VCR following instructions and recording your favourite show - forget about it.All ...1 week ago
Do you remember Y2K, the threat that hung over humanity in the closing days of the twentieth century? Horror scenarios of planes falling from the sky, electronic payments failing and ATMs refusing to dispense cash. As for your VCR following instructions and recording your favourite show - forget about it.All ...1 week ago - Bernard’s Saturday Soliloquy for the week to July 20
 Climate Change Minister Simon Watts being questioned by The Kākā’s Bernard Hickey.TL;DR: My top six things to note around housing, climate and poverty in Aotearoa’s political economy in the week to July 20 were:1. A strategy that fails Zero Carbon Act & Paris targetsThe National-ACT-NZ First Coalition Government finally unveiled ...1 week ago
Climate Change Minister Simon Watts being questioned by The Kākā’s Bernard Hickey.TL;DR: My top six things to note around housing, climate and poverty in Aotearoa’s political economy in the week to July 20 were:1. A strategy that fails Zero Carbon Act & Paris targetsThe National-ACT-NZ First Coalition Government finally unveiled ...1 week ago - Pharmac Director, Climate Change Commissioner, Health NZ Directors – The latest to quit this m...
 Summary:As New Zealand loses at least 12 leaders in the public service space of health, climate, and pharmaceuticals, this month alone, directly in response to the Government’s policies and budget choices, what lies ahead may be darker than it appears. Tui examines some of those departures and draws a long ...1 week ago
Summary:As New Zealand loses at least 12 leaders in the public service space of health, climate, and pharmaceuticals, this month alone, directly in response to the Government’s policies and budget choices, what lies ahead may be darker than it appears. Tui examines some of those departures and draws a long ...1 week ago - Flooding Housing Policy
 The Minister of Housing’s ambition is to reduce markedly the ratio of house prices to household incomes. If his strategy works it would transform the housing market, dramatically changing the prospects of housing as an investment.Leaving aside the Minister’s metaphor of ‘flooding the market’ I do not see how the ...1 week ago
The Minister of Housing’s ambition is to reduce markedly the ratio of house prices to household incomes. If his strategy works it would transform the housing market, dramatically changing the prospects of housing as an investment.Leaving aside the Minister’s metaphor of ‘flooding the market’ I do not see how the ...1 week ago - A Voyage Among the Vandals: Accepted (Again!)
 As previously noted, my historical fantasy piece, set in the fifth-century Mediterranean, was accepted for a Pirate Horror anthology, only for the anthology to later fall through. But in a good bit of news, it turned out that the story could indeed be re-marketed as sword and sorcery. As of ...1 week ago
As previously noted, my historical fantasy piece, set in the fifth-century Mediterranean, was accepted for a Pirate Horror anthology, only for the anthology to later fall through. But in a good bit of news, it turned out that the story could indeed be re-marketed as sword and sorcery. As of ...1 week ago - The Kākā's Chorus for Friday, July 19
 An employee of tobacco company Philip Morris International demonstrates a heated tobacco device. Photo: Getty ImagesTL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy on Friday, July 19 are:At a time when the Coalition Government is cutting spending on health, infrastructure, education, housing ...1 week ago
An employee of tobacco company Philip Morris International demonstrates a heated tobacco device. Photo: Getty ImagesTL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy on Friday, July 19 are:At a time when the Coalition Government is cutting spending on health, infrastructure, education, housing ...1 week ago - The Kākā’s Pick 'n' Mix for Friday, July 19
 TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 8:30 am on Friday, July 19 are:Scoop: NZ First Minister Casey Costello orders 50% cut to excise tax on heated tobacco products. The minister has ...1 week ago
TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 8:30 am on Friday, July 19 are:Scoop: NZ First Minister Casey Costello orders 50% cut to excise tax on heated tobacco products. The minister has ...1 week ago - Weekly Roundup 19-July-2024
Kia ora, it’s time for another Friday roundup, in which we pull together some of the links and stories that caught our eye this week. Feel free to add more in the comments! Our header image this week shows a foggy day in Auckland town, captured by Patrick Reynolds. ...1 week ago
- Weekly Climate Wrap: A market-led plan for failure
TL;DR : Here’s the top six items climate news for Aotearoa this week, as selected by Bernard Hickey and The Kākā’s climate correspondent Cathrine Dyer. A discussion recorded yesterday is in the video above and the audio of that sent onto the podcast feed.The Government released its draft Emissions Reduction ...1 week ago
- Tobacco First
 Save some money, get rich and old, bring it back to Tobacco Road.Bring that dynamite and a crane, blow it up, start all over again.Roll up. Roll up. Or tailor made, if you prefer...Whether you’re selling ciggies, digging for gold, catching dolphins in your nets, or encouraging folks to flutter ...1 week ago
Save some money, get rich and old, bring it back to Tobacco Road.Bring that dynamite and a crane, blow it up, start all over again.Roll up. Roll up. Or tailor made, if you prefer...Whether you’re selling ciggies, digging for gold, catching dolphins in your nets, or encouraging folks to flutter ...1 week ago - Trump’s Adopted Son.
 Waiting In The Wings: For truly, if Trump is America’s un-assassinated Caesar, then J.D. Vance is America’s Octavian, the Republic’s youthful undertaker – and its first Emperor.DONALD TRUMP’S SELECTION of James D. Vance as his running-mate bodes ill for the American republic. A fervent supporter of Viktor Orban, the “illiberal” prime ...1 week ago
Waiting In The Wings: For truly, if Trump is America’s un-assassinated Caesar, then J.D. Vance is America’s Octavian, the Republic’s youthful undertaker – and its first Emperor.DONALD TRUMP’S SELECTION of James D. Vance as his running-mate bodes ill for the American republic. A fervent supporter of Viktor Orban, the “illiberal” prime ...1 week ago - The Kākā’s Journal of Record for Friday, July 19
 TL;DR: As of 6:00 am on Friday, July 19, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:The PSA announced the Employment Relations Authority (ERA) had ruled in the PSA’s favour in its case against the Ministry ...1 week ago
TL;DR: As of 6:00 am on Friday, July 19, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:The PSA announced the Employment Relations Authority (ERA) had ruled in the PSA’s favour in its case against the Ministry ...1 week ago
{kind=link}
- Release: Charter schools to remove the rights of teachers
 A late change to charter school legislation will cheat educators out of fair pay and negotiating power proving charter schools are just a vehicle to make profit out of our education system. ...23 hours ago
A late change to charter school legislation will cheat educators out of fair pay and negotiating power proving charter schools are just a vehicle to make profit out of our education system. ...23 hours ago - Te iwi Māori will not stand for another Foreshore and Seabed
In 2004 te iwi Māori rallied against the Crown’s attempt to confiscate our coastlines and moana with the Foreshore and Seabed Act. This led to the largest hīkoi of a generation and the birth of Te Pāti Māori. 20 years later, history is repeating itself. Today the government has announced ...2 days ago
- Te Pāti Māori Acknowledge the Need for Fundamental Change in State Care
It has been five and a half years since the Royal Commission of Inquiry into Abuse in Care was established to investigate the abuse of children, young people, and vulnerable adults within state and faith-based institutions. Yesterday, the final report - Whanaketia through pain and trauma, from darkness to light ...2 days ago
- Release: National disgrace for children in poverty
Shifting the goalposts on child poverty is a new low for the National-led government. ...2 days ago
- National disgrace for children in poverty
Shifting the goalposts on child poverty is a new low for the National-led government. ...2 days ago
- Government quietly waters down child poverty targets
 The Government’s move to dilute child poverty targets is a reminder that it is actively choosing to preserve hardship for thousands of households. ...2 days ago
The Government’s move to dilute child poverty targets is a reminder that it is actively choosing to preserve hardship for thousands of households. ...2 days ago - Release: National jumps on Labour’s trains
National is so short on ideas it is now announcing Labour’s rail announcement from a year ago, Labour transport spokesperson Tangi Utikere said. ...2 days ago
- Release: Opposition parties unite to protect ECE
Labour, the Green Party and Te Pāti Māori are uniting to stop the Government’s dangerous changes to the Early Childhood Education sector. ...2 days ago
- Release: Another step forward for survivors of abuse in care
Labour welcomes the Royal Commission of Inquiry into Abuse in Care’s final report and the government committing to a formal apology in November. ...3 days ago
- Govt must listen to experiences of abuse survivors
The Government must do all it can to bring abuse in care to an end following the release of the independent inquiry. ...3 days ago
- Release: Health New Zealand exposes Minister spinning in freefall
Health New Zealand contradicted the Government’s spin that back-office bureaucracy is the cause of overspend in the public health system. ...4 days ago
- Govt must act on Israel’s illegal occupation of Palestine
The Green Party is calling on the Government to take action off the back of the International Court of Justice ruling on Israel’s illegal occupation of Palestine. ...4 days ago
- NZ Government Must Enforce ICJ Ruling
On Friday the International Court of Justice reaffirmed what Palestinian’s have been telling us for decades: that the occupation and colonisation of Palestinian lands by Israel is illegal and must end immediately. They also called for reparations for Palestinian’s who have lived under Israeli occupation since it began in 1967. ...5 days ago
- Release: Listen PM, boot camps don’t work
Refusing to listen to evidence, experts or experience the Government is stubbornly marching ahead with its boot camps. ...7 days ago
- Release: Govt must act on ICJ ruling on illegal Israeli occupation
Labour calls on the Government to act after the International Court of Justice (ICJ) ruled that Israel’s occupation of Palestinian Territories is illegal. ...7 days ago
- Release: Rents up under National, promises fall flat
National Party policies which promised to put “downward pressure” on rents are having the opposite effect. ...1 week ago
- MSD figures show Govt determined to punish beneficiaries
The 53.7 percent rise in benefit sanctions over the last year is more proof of this Government’s disdain for our communities most in need of support. ...1 week ago
- We need real solutions, not more failed boot camps – Willow-Jean Prime
Aotearoa could be a country where every child grows up feeling safe, loved and with a sense of belonging in their whānau and community. But for some of our children, this is far from reality. Instead, they are trapped in a maze of intergenerational harm that they can’t escape on ...1 week ago
- David Seymour is Unfit to Serve as Minister
Te Pāti Māori are calling for David Seymour to resign as Associate Health Minister in response to his call for Pharmac to ignore the Treaty of Waitangi. “This announcement is just another example of the government’s anti-Tiriti, anti-Māori agenda.” Said Co-leader and spokesperson for health, Debbie Ngarewa-Packer. “Seymour thinks it ...1 week ago
- Renters suffer as soaring rents feed rising inflation
The soaring price of renting is driving the rise of inflation in this country - with latest figures from Stats NZ showing rents are up 4.8 per cent on average while annual inflation is at 3.3 per cent. ...1 week ago
- National’s climate strategy undoes good progress
National’s Emissions Reduction Plan will take New Zealand further from the economy we need to ensure the next generation has a stable climate and secure livelihoods. ...1 week ago
- Green Party releases executive summary of independent investigation
Following consultation with named parties and thorough consideration of privacy interests, the Green Party is in a position to release the Executive Summary of the final report from the independent investigation into Darleen Tana. ...1 week ago
- Government back off track on climate action
Today’s Draft Emissions Reduction Plan shows the Government couldn’t care less about a liveable climate for all. ...1 week ago
- PM needs to step in over Shane Jones’ undeclared meeting
Prime Minister Christopher Luxon should be asking serious questions of his Minister for Resources Shane Jones now it’s been revealed he misled the public about a dinner with mining companies that he didn’t declare and said wasn’t pre-arranged. ...2 weeks ago
- Te Pāti Māori Opposes Three Strikes Amendment Bill
Te Pāti Māori have submitted to the Justice Select Committee against the Sentencing (Reinstating Three Strikes) Amendment Bill. The bill will further entrench racism in our justice system and fails to focus on rehabilitation. “Reinstating Three Strikes will empower a systematically racist system and exacerbate the overrepresentation of Māori in ...2 weeks ago
- Govt Determined to Make Aotearoa a Country of Disposable Renters
The Transport and Infrastructure Committee is set to make a determination on the Residential Tenancies Amendment (RTA) Bill in the coming weeks. “This legislation will give landlords the power to kick our whānau out onto the street for no reason” said Housing spokesperson, Mariameno Kapa-Kingi. “Their solution to the housing ...2 weeks ago
- Statement on retail crime Ministerial Advisory Group
“National’s campaign was about tackling crime and the best they can do is a two-year long Ministerial Advisory Group,” Labour justice spokesperson Duncan Webb said. ...2 weeks ago
- Statement from Labour education spokesperson Jan Tinetti
“There are more examples of charter schools failing their students than there are success stories. The coalition Government is driving to dismantle our public school system and instead promote a privatised, competitive structure that puts profits before kids,” Jan Tinetti said. ...2 weeks ago
- Govt Continues to Destructively Withhold Information
“This government is choosing to deliberately mislead and withhold information, keeping our people in the dark about this government’s agenda and the future of our mokopuna,” said co-leader and spokesperson for Health, Debbie Ngarewa-Packer. The call comes after the demand from the Chief Ombudsman that Associate Minister of Health, Casey ...2 weeks ago
- Statement from Labour climate change spokesperson Megan Woods
“Today’s climate announcement by Simon Watts makes clear the National Government is simply paying lip service to meeting its climate change targets,” Megan Woods said. ...2 weeks ago
- Eight ways National is making life harder for workers
National is choosing to make life harder for workers by taking away the rights our communities have fought hard for. Here's how they’re taking workers backwards. ...3 weeks ago
- Waitlists up and workforce down under National
Health New Zealand’s recent quarterly performance report shows the public health system is going backwards under the National government. ...3 weeks ago
- Joint statement from the Prime Ministers of Canada, Australia and New Zealand
 Australia, Canada and New Zealand today issued the following statement on the need for an urgent ceasefire in Gaza and the risk of expanded conflict between Hizballah and Israel. The situation in Gaza is catastrophic. The human suffering is unacceptable. It cannot continue. We remain unequivocal in our condemnation of ...17 hours ago
Australia, Canada and New Zealand today issued the following statement on the need for an urgent ceasefire in Gaza and the risk of expanded conflict between Hizballah and Israel. The situation in Gaza is catastrophic. The human suffering is unacceptable. It cannot continue. We remain unequivocal in our condemnation of ...17 hours ago - AG reminds institutions of legal obligations
Attorney-General Judith Collins today reminded all State and faith-based institutions of their legal obligation to preserve records relevant to the safety and wellbeing of those in its care. “The Abuse in Care Inquiry’s report has found cases where records of the most vulnerable people in State and faith‑based institutions were ...20 hours ago
- More young people learning about digital safety
Minister of Internal Affairs Brooke van Velden says the Government’s online safety website for children and young people has reached one million page views. “It is great to see so many young people and their families accessing the site Keep It Real Online to learn how to stay safe online, and manage ...20 hours ago
- Speech to the Conference for General Practice 2024
Tēnā tātou katoa, Ngā mihi te rangi, ngā mihi te whenua, ngā mihi ki a koutou, kia ora mai koutou. Thank you for the opportunity to be here and the invitation to speak at this 50th anniversary conference. I acknowledge all those who have gone before us and paved the ...23 hours ago
- Employers and payroll providers ready for tax changes
New Zealand’s payroll providers have successfully prepared to ensure 3.5 million individuals will, from Wednesday next week, be able to keep more of what they earn each pay, says Finance Minister Nicola Willis and Revenue Minister Simon Watts. “The Government's tax policy changes are legally effective from Wednesday. Delivering this tax ...1 day ago
- Experimental vineyard futureproofs wine industry
An experimental vineyard which will help futureproof the wine sector has been opened in Blenheim by Associate Regional Development Minister Mark Patterson. The covered vineyard, based at the New Zealand Wine Centre – Te Pokapū Wāina o Aotearoa, enables controlled environmental conditions. “The research that will be produced at the Experimental ...1 day ago
- Funding confirmed for regions affected by North Island Weather Events
The Coalition Government has confirmed the indicative regional breakdown of North Island Weather Event (NIWE) funding for state highway recovery projects funded through Budget 2024, Transport Minister Simeon Brown says. “Regions in the North Island suffered extensive and devastating damage from Cyclone Gabrielle and the 2023 Auckland Anniversary Floods, and ...1 day ago
- Indonesian Foreign Minister to visit
Indonesia’s Foreign Minister, Retno Marsudi, will visit New Zealand next week, Foreign Minister Winston Peters has announced. “Indonesia is important to New Zealand’s security and economic interests and is our closest South East Asian neighbour,” says Mr Peters, who is currently in Laos to engage with South East Asian partners. ...1 day ago
- Strengthening partnership with Ngāti Maniapoto
He aha te kai a te rangatira? He kōrero, he kōrero, he kōrero. The government has reaffirmed its commitment to supporting the aspirations of Ngāti Maniapoto, Minister for Māori Development Tama Potaka says. “My thanks to Te Nehenehenui Trust – Ngāti Maniapoto for bringing their important kōrero to a ministerial ...2 days ago
- Transport Minister thanks outgoing CAA Chair
Transport Minister Simeon Brown has thanked outgoing Chair of the Civil Aviation Authority, Janice Fredric, for her service to the board.“I have received Ms Fredric’s resignation from the role of Chair of the Civil Aviation Authority,” Mr Brown says.“On behalf of the Government, I want to thank Ms Fredric for ...2 days ago
- Test for Customary Marine Title being restored
The Government is proposing legislation to overturn a Court of Appeal decision and amend the Marine and Coastal Area Act in order to restore Parliament’s test for Customary Marine Title, Treaty Negotiations Minister Paul Goldsmith says. “Section 58 required an applicant group to prove they have exclusively used and occupied ...2 days ago
- Opposition united in bad faith over ECE sector review
Regulation Minister David Seymour says that opposition parties have united in bad faith, opposing what they claim are ‘dangerous changes’ to the Early Childhood Education sector, despite no changes even being proposed yet. “Issues with affordability and availability of early childhood education, and the complexity of its regulation, has led ...2 days ago
- Kiwis having their say on first regulatory review
After receiving more than 740 submissions in the first 20 days, Regulation Minister David Seymour is asking the Ministry for Regulation to extend engagement on the early childhood education regulation review by an extra two weeks. “The level of interest has been very high, and from the conversations I’ve been ...2 days ago
- Government upgrading Lower North Island commuter rail
The Coalition Government is investing $802.9 million into the Wairarapa and Manawatū rail lines as part of a funding agreement with the NZ Transport Agency (NZTA), KiwiRail, and the Greater Wellington and Horizons Regional Councils to deliver more reliable services for commuters in the lower North Island, Transport Minister Simeon ...2 days ago
- Government moves to ensure flood protection for Wairoa
Local Government Minister Simeon Brown has announced his intention to appoint a Crown Manager to both Hawke’s Bay Regional and Wairoa District Councils to speed up the delivery of flood protection work in Wairoa."Recent severe weather events in Wairoa this year, combined with damage from Cyclone Gabrielle in 2023 have ...3 days ago
- PM speech to Parliament – Royal Commission of Inquiry’s Report into Abuse in Care
Mr Speaker, this is a day that many New Zealanders who were abused in State care never thought would come. It’s the day that this Parliament accepts, with deep sorrow and regret, the Report of the Royal Commission of Inquiry into Abuse in Care. At the heart of this report are the ...3 days ago
- Government acknowledges torture at Lake Alice
For the first time, the Government is formally acknowledging some children and young people at Lake Alice Psychiatric Hospital experienced torture. The final report of the Royal Commission of Inquiry into Abuse in State and Faith-based Care “Whanaketia – through pain and trauma, from darkness to light,” was tabled in Parliament ...3 days ago
- Government acknowledges courageous abuse survivors
The Government has acknowledged the nearly 2,400 courageous survivors who shared their experiences during the Royal Commission of Inquiry into Historical Abuse in State and Faith-Based Care. The final report from the largest and most complex public inquiry ever held in New Zealand, the Royal Commission Inquiry “Whanaketia – through ...3 days ago
- Half a million people use tax calculator
With a week to go before hard-working New Zealanders see personal income tax relief for the first time in fourteen years, 513,000 people have used the Budget tax calculator to see how much they will benefit, says Finance Minister Nicola Willis. “Tax relief is long overdue. From next Wednesday, personal income ...3 days ago
- Paid Parental Leave improvements pass first reading
Workplace Relations and Safety Minister Brooke van Velden says a bill that has passed its first reading will improve parental leave settings and give non-biological parents more flexibility as primary carer for their child. The Regulatory Systems Amendment Bill (No3), passed its first reading this morning. “It includes a change ...3 days ago
- Rebuilding the economy through better regulation
Two Bills designed to improve regulation and make it easier to do business have passed their first reading in Parliament, says Economic Development Minister Melissa Lee. The Regulatory Systems (Economic Development) Amendment Bill and Regulatory Systems (Immigration and Workforce) Amendment Bill make key changes to legislation administered by the Ministry ...3 days ago
- ‘Open banking’ and ‘open electricity’ on the way
New legislation paves the way for greater competition in sectors such as banking and electricity, Commerce and Consumer Affairs Minister Andrew Bayly says. “Competitive markets boost productivity, create employment opportunities and lift living standards. To support competition, we need good quality regulation but, unfortunately, a recent OECD report ranked New ...3 days ago
- Charity lotteries to be permitted to operate online
Minister of Internal Affairs Brooke van Velden says lotteries for charitable purposes, such as those run by the Heart Foundation, Coastguard NZ, and local hospices, will soon be allowed to operate online permanently. “Under current laws, these fundraising lotteries are only allowed to operate online until October 2024, after which ...4 days ago
- Accelerating Northland Expressway
The Coalition Government is accelerating work on the new four-lane expressway between Auckland and Whangārei as part of its Roads of National Significance programme, with an accelerated delivery model to deliver this project faster and more efficiently, Transport Minister Simeon Brown says. “For too long, the lack of resilient transport connections ...4 days ago
- Sir Don to travel to Viet Nam as special envoy
Sir Don McKinnon will travel to Viet Nam this week as a Special Envoy of the Government, Foreign Minister Winston Peters has announced. “It is important that the Government give due recognition to the significant contributions that General Secretary Nguyen Phu Trong made to New Zealand-Viet Nam relations,” Mr ...4 days ago
- Grant Illingworth KC appointed as transitional Commissioner to Royal Commission
Minister of Internal Affairs Brooke van Velden says newly appointed Commissioner, Grant Illingworth KC, will help deliver the report for the first phase of the Royal Commission of Inquiry into COVID-19 Lessons, due on 28 November 2024. “I am pleased to announce that Mr Illingworth will commence his appointment as ...4 days ago
- NZ to advance relationships with ASEAN partners
Foreign Minister Winston Peters travels to Laos this week to participate in a series of Association of Southeast Asian Nations (ASEAN)-led Ministerial meetings in Vientiane. “ASEAN plays an important role in supporting a peaceful, stable and prosperous Indo-Pacific,” Mr Peters says. “This will be our third visit to ...4 days ago
- Backing mental health services on the West Coast
Construction of a new mental health facility at Te Nikau Grey Hospital in Greymouth is today one step closer, Mental Health Minister Matt Doocey says. “This $27 million facility shows this Government is delivering on its promise to boost mental health care and improve front line services,” Mr Doocey says. ...4 days ago
- NZ support for sustainable Pacific fisheries
New Zealand is committing nearly $50 million to a package supporting sustainable Pacific fisheries development over the next four years, Foreign Minister Winston Peters and Oceans and Fisheries Minister Shane Jones announced today. “This support consisting of a range of initiatives demonstrates New Zealand’s commitment to assisting our Pacific partners ...4 days ago
- Students’ needs at centre of new charter school adjustments
Associate Education Minister David Seymour says proposed changes to the Education and Training Amendment Bill will ensure charter schools have more flexibility to negotiate employment agreements and are equipped with the right teaching resources. “Cabinet has agreed to progress an amendment which means unions will not be able to initiate ...4 days ago
- Commissioner replaces Health NZ Board
In response to serious concerns around oversight, overspend and a significant deterioration in financial outlook, the Board of Health New Zealand will be replaced with a Commissioner, Health Minister Dr Shane Reti announced today. “The previous government’s botched health reforms have created significant financial challenges at Health NZ that, without ...5 days ago
- Minister to speak at Australian Space Forum
Minister for Space and Science, Innovation and Technology Judith Collins will travel to Adelaide tomorrow for space and science engagements, including speaking at the Australian Space Forum. While there she will also have meetings and visits with a focus on space, biotechnology and innovation. “New Zealand has a thriving space ...5 days ago
- Climate Change Minister to attend climate action meeting in China
Climate Change Minister Simon Watts will travel to China on Saturday to attend the Ministerial on Climate Action meeting held in Wuhan. “Attending the Ministerial on Climate Action is an opportunity to advocate for New Zealand climate priorities and engage with our key partners on climate action,” Mr Watts says. ...5 days ago
- Oceans and Fisheries Minister to Solomons
Oceans and Fisheries Minister Shane Jones is travelling to the Solomon Islands tomorrow for meetings with his counterparts from around the Pacific supporting collective management of the region’s fisheries. The 23rd Pacific Islands Forum Fisheries Committee and the 5th Regional Fisheries Ministers’ Meeting in Honiara from 23 to 26 July ...7 days ago
- Government launches Military Style Academy Pilot
The Government today launched the Military Style Academy Pilot at Te Au rere a te Tonga Youth Justice residence in Palmerston North, an important part of the Government’s plan to crackdown on youth crime and getting youth offenders back on track, Minister for Children, Karen Chhour said today. “On the ...7 days ago
- Nine priority bridge replacements to get underway
The Government has welcomed news the NZ Transport Agency (NZTA) has begun work to replace nine priority bridges across the country to ensure our state highway network remains resilient, reliable, and efficient for road users, Transport Minister Simeon Brown says.“Increasing productivity and economic growth is a key priority for the ...1 week ago
- Update on global IT outage
Acting Prime Minister David Seymour has been in contact throughout the evening with senior officials who have coordinated a whole of government response to the global IT outage and can provide an update. The Department of the Prime Minister and Cabinet has designated the National Emergency Management Agency as the ...1 week ago
- New Zealand, Japan renew Pacific partnership
New Zealand and Japan will continue to step up their shared engagement with the Pacific, Foreign Minister Winston Peters says. “New Zealand and Japan have a strong, shared interest in a free, open and stable Pacific Islands region,” Mr Peters says. “We are pleased to be finding more ways ...1 week ago
- New infrastructure energises BOP forestry towns
New developments in the heart of North Island forestry country will reinvigorate their communities and boost economic development, Regional Development Minister Shane Jones says. Mr Jones visited Kaingaroa and Kawerau in Bay of Plenty today to open a landmark community centre in the former and a new connecting road in ...1 week ago
- 'Pacific Futures'
President Adeang, fellow Ministers, honourable Diet Member Horii, Ambassadors, distinguished guests. Minasama, konnichiwa, and good afternoon, everyone. Distinguished guests, it’s a pleasure to be here with you today to talk about New Zealand’s foreign policy reset, the reasons for it, the values that underpin it, and how it ...1 week ago
- 'Enough is enough' – Chris Hipkins blasts government over Māori policies
 Labour Party leader Chris Hipkins says the coalition government is unfairly targeting Māori: "Each week they find new ways to keep Māori down." ...1 hour ago
Labour Party leader Chris Hipkins says the coalition government is unfairly targeting Māori: "Each week they find new ways to keep Māori down." ...1 hour ago - Focus on Politics: Abuse in care report delivers demands for justice
The government has promised to listen to survivors, but how it responds and whether justice is served remains to be seen. ...6 hours ago
- Green AGM: Party processes will be respected on Darleen Tana issue, Chlöe Swarbrick says
A Green Party member is concerned that proper process will not be followed - but the party's co-leader says a vote will not be forced. ...6 hours ago
- Short story: Fire Engines, by Gina Butson
 Last summer when Matairangi burned, Ginny and Tom stood at the window of their lounge, watching kākā shoot skyward from the burning trees. From the distance, they looked to Ginny like pages torn from books and thrown into a bonfire. It was Tom, voice tight, who told her it was ...6 hours ago
Last summer when Matairangi burned, Ginny and Tom stood at the window of their lounge, watching kākā shoot skyward from the burning trees. From the distance, they looked to Ginny like pages torn from books and thrown into a bonfire. It was Tom, voice tight, who told her it was ...6 hours ago - Alice Munro’s shocking silence
Opinion: The Canadian short story writer Alice Munro – winner of the Nobel Prize in Literature in 2013 – died in May at the age of 92. Her work was about “the damage people inflict on one another in the name of love”, Deborah Treisman wrote in the New Yorker. ...6 hours ago
- Re-writing the timeline of the universe
This month marks two years since the most powerful telescope ever built sent its first pictures back to earth. From its lofty vantage point, beyond the moon in orbit around the sun, the James Webb Space Telescope was tuned to observe the first stars and galaxies being born soon after ...6 hours ago
- Anne Salmond: What track was that?
Comment: After Climate Change Minister Simon Watts’ preview several weeks ago, I had some optimism about the Government’s emissions reduction plan. Now I’ve read the discussion document, that hope has been dashed. How can the Government propose a plan that wants to take New Zealand taxpayers’ hard-earned money, and spend ...6 hours ago
- The Secret Diary of .. NZ’s Olympics hopefuls
Christopher Luxon: hurdles The little man from National jumps hurdles in his sleep. He’s quite good at it in his dreams and even though the reality doesn’t quite match up you have to give him credit for getting up every morning and crashing into the very first hurdle of the ...6 hours ago
- Finally heard, seen – and believed
Comment: It was a good two hours into the conversation when Tyrone Marks raised the most basic of questions when I first spoke to him in 2017. “They didn’t explain the things they did to me. They never told me why. And they still haven’t. There’s no explanation for it. ...6 hours ago
- The Weekend: If in doubt, go to the funeral
 Madeleine Chapman rounds out Death Week on The Spinoff with a final recommendation. You can read all of our Death Week coverage here. Nothing forces you to reflect on your life and relationships quite like proximity to death. For those whose nearest and dearest have died, there are reasonably obvious ...7 hours ago
Madeleine Chapman rounds out Death Week on The Spinoff with a final recommendation. You can read all of our Death Week coverage here. Nothing forces you to reflect on your life and relationships quite like proximity to death. For those whose nearest and dearest have died, there are reasonably obvious ...7 hours ago - ‘What a privilege’: Whitney from The Traitors NZ on life as a funeral director
Whitney Greene takes us through her life in television, including the TV character she’d like to plan a funeral for and her cow lung catastrophe on The Traitors NZ. “If the phone rings, I have to answer it,” Whitney Greene from The Traitors NZ warns as we begin our My ...7 hours ago
- Rich and rare: Bad Archive by Flora Feltham, reviewed
Maddie Ballard reviews the debut essay collection of Pōneke writer Flora Feltham. In ‘The Raw Material’, the longest essay in Flora Feltham’s dazzling debut collection, the author heads out for a run after hours of weaving and sees the world turn to textile. “Pounding along the Parade, I saw the ...7 hours ago
- ‘Possibly the best live gig I have been to’: TRiPS’ perfect weekend playlist
Andy Christiansen, one half of the experimental rock-pop duo TRiPS, shares the tunes inspiring the band’s perfect weekend and new release. “Good speakers, good food, good music, no distractions”: that’s all you need to enjoy the psychedelic stylings of TRiPS, a new band formed by Fly My Pretties’ Barnaby Weir ...7 hours ago
- Every sport at the Paris Olympics, ranked from least to most fun to watch
Celebrating our quadrennial opportunity to become experts in a bunch of sports we never normally watch. The games of the XXXIII Olympiad are upon us. Paris will host this year’s showcase of sporting and athletic prowess, which means some late-night and early-morning viewing for us in Aotearoa. But what sports ...7 hours ago
- The Sunday Essay: Remembering my brother
The photograph is striking and beautiful, but also disturbing – a reminder that my love for John was often entangled in shame. The Sunday Essay is made possible thanks to the support of Creative New Zealand. In the spring of 1980, in Dunedin, shortly before his death, someone took a photograph ...7 hours ago
- Dog of the month: Babushka, who is notorious in Newtown
Get to know Babushka, our latest Dog of the Month. This feature was offered as a reward during our What’s Eating Aotearoa PledgeMe campaign. Thank you to Babu’s humans, Jo and Isabel, for their support. Dog name: Babushka (Babu for short) Age: 2 Breed: Border Collie X poodle If rescued, ...7 hours ago
- Photojournalist targeted by Israeli army carries Olympic torch in Paris
 Pacific Media Watch A Lebanese photojournalist who was severely wounded during an Israeli air strike in south Lebanon carried the Olympic torch in Paris this week in honour of her peers who have been wounded and killed in the field — especially in Gaza and Lebanon. Christina Assi of Agence ...14 hours ago
Pacific Media Watch A Lebanese photojournalist who was severely wounded during an Israeli air strike in south Lebanon carried the Olympic torch in Paris this week in honour of her peers who have been wounded and killed in the field — especially in Gaza and Lebanon. Christina Assi of Agence ...14 hours ago - 70 years on from tests, Marshallese women still fight for nuclear justice
The first report in a five-part web series focused on the 15th Triennial Conference of Pacific Women taking place in the Marshall Islands this week. SPECIAL REPORT: By Netani Rika in Majuro Women continue to fight for justice 70 years after the first nuclear tests by the United States caused ...15 hours ago
- 'Israel must listen' – Luxon, Albanese, Trudeau issue joint support for US-backed ce...
Christopher Luxon has joined with Australia and Canada's leaders in voicing support for US President Joe Biden's ceasefire deal between Israel and Hamas. ...16 hours ago
- Politics with Michelle Grattan: ‘Teal’ Zoe Daniel on political donations, representing Jewish vo...
Source: The Conversation (Au and NZ) – By Michelle Grattan, Professorial Fellow, University of Canberra The 2022 election brought the “teal wave” into parliament. The next election will test whether teals, who occupy what were Liberal seats, and other independents can maintain their momentum. Joining us on the Podcast ...17 hours ago
- China: still the world’s biggest emitter, but also an emerging force in climate diplomacy
Source: The Conversation (Au and NZ) – By Xu Yi-chong, Professor of Governance and Public Policy, Griffith University fuyu liu, Shutterstock Seven years seems a lifetime in politics. In 2017, President Donald Trump announced the United States would withdraw from the Paris Agreement. It prompted Canada, China and the ...17 hours ago
- Federal Court finds insufficient evidence Roundup weedkiller causes cancer. What does the science sa...
Source: The Conversation (Au and NZ) – By Ian Musgrave, Senior lecturer in Pharmacology, University of Adelaide Pixavri/Shutterstock A major Federal Court class action has been dismissed this week after Justice Michael Lee ruled there was not enough evidence to prove the weedkiller Roundup causes cancer. Plaintiff Kelvin ...17 hours ago
- The Week in Politics: Parliament set a vital task, Darleen Tana returns
In The Week in Politics: politicians have to decide what to do about child abuse, Health NZ is booked in for major surgery and Darleen Tana returns. ...17 hours ago
- Māori leader says government's controversial boot camps the wrong approach
Meihana Durie is concerned a camp draws from methodology popularised by the US marines. ...18 hours ago
- Twice as good for half the respect: Kamala Harris’ battle for the White House
Source: The Conversation (Au and NZ) – By Clare Corbould, Associate Professor, Contemporary Histories Research Group, Deakin University Mainstream media are surprisingly muted at the prospect of the world’s most powerful nation being led for the first time by a woman – specifically a woman of colour, Vice President Kamala ...18 hours ago
- Drone food delivery is spreading across Australia. Research suggests we will eat more junk food as a...
Source: The Conversation (Au and NZ) – By Rebecca Bennett, PhD Student, Associate Research Fellow, Deakin University Last week, a drone delivery company called Wing (owned by Google’s parent company, Alphabet) started operating in Melbourne. Some 250,000 residents in parts of the city’s eastern suburbs can now order food from ...18 hours ago
- Our research shows 4 in 10 Australians in aged care are malnourished. What can we do about it?
Source: The Conversation (Au and NZ) – By Jonathan Foo, Lecturer, Physiotherapy, Monash University pikselstock/Shutterstock In the next 40 years in Australia, it’s predicted the number of Australians aged 65 and over will more than double, while the number of people aged 85 and over will more than triple. ...18 hours ago
- Before there was diving and relays, there was the Poetry Olympics
Source: The Conversation (Au and NZ) – By Katrina Grant, Research Associate, Power Institute for Arts and Visual Culture, University of Sydney Jonas Åkerström’s 1790 work, Session of the Accademia dell’Arcadia on August 17 1788. Nationalmuseum/Cecilia Heisser Ever wondered whether you’d have a better chance at winning an Olympic gold ...19 hours ago
- Abuse in Care inquiry: Judith Collins warns of possible prosecutions if records destroyed
Judith Collins is reminding all state and faith-based institutions of their legal obligation to preserve records. ...19 hours ago
- Health star labels move closer to being mandatory. But food companies could still (legally) game the...
Source: The Conversation (Au and NZ) – By Alexandra Jones, Program Lead, Food Governance, George Institute for Global Health wavebreakmedia/Shutterstock On Thursday, Australian and New Zealand food ministers at state, federal and national levels met to thrash out what’s next for health star ratings on packaged foods. Now, after ...20 hours ago
- Abuse in Care inquiry: Call for Pacific focused redress pathway
The Abuse in Care report found many Pacific survivors lost their connections to their culture and language, resulting in trauma that has been carried from generation to generation. ...21 hours ago
- Education Review Office Pragmatism Will Really Help The Sector While The Regulation Review Is Underw...
 In the regulatory review, ECC intends to suggest that ERO focus on curriculum delivery reviews rather than the Ministry, because it’s not efficient or effective to have two agencies with radically different approaches climbing over each other. ...21 hours ago
In the regulatory review, ECC intends to suggest that ERO focus on curriculum delivery reviews rather than the Ministry, because it’s not efficient or effective to have two agencies with radically different approaches climbing over each other. ...21 hours ago - Watch: Christopher Luxon's security cut short visit ahead of protest
The prime minister was speaking to reporters during a walkabout with police in central Auckland. ...22 hours ago
- Christopher Luxon calls for witnesses to alleged '80s politician paedophile ring to speak out
Christopher Luxon says anyone with evidence about claims involving politicians and civil servants in the 1980s should go to police. ...22 hours ago
- Co-chairs Of Te Rūnanga Nui O Ngā Kura Kaupapa Māori Welcome The Waitangi Tribunal Report –...
Te Rūnanga Nui o Ngā Kura Kaupapa Māori invites the current government to work in partnership with them to develop a pathway forward, including the development of a parallel pathway and meaningful policy and strategy for Kura Kaupapa Māori ...22 hours ago
- Why this season of The Traitors is the best reality TV NZ has ever made
If you haven’t started watching yet, Tara Ward begs you to reconsider. This is an excerpt from our weekly pop culture newsletter Rec Room. Sign up here. In the world of New Zealand reality television, we have many gems in our crown. There’s the delicious second season of the Celebrity Treasure ...22 hours ago
- The Friday Poem: ‘The clothes of the dead’ by Fiona Kidman
A new poem by Fiona Kidman. The clothes of the dead I did not keep my mother’s furry red beret for long nor the stringy scarves that adorned the necks of my aunts, although I have kept tag ends of gold, the rings and trinkets they wore, the brooches no ...22 hours ago
- Ngāi Tahu Challenges Changes To MACA
The government’s announcement that it will re-open the foreshore and seabed controversy by changing the rules on recognising centuries-old Māori customary title for a third time goes against the rule of law and New Zealand values,” Mr Tipa says. ...22 hours ago
- The Unity Books bestseller chart for the week ending July 26
The only published and available best-selling indie book chart in New Zealand is the top 10 sales list recorded every week at Unity Books’ stores in High St, Auckland, and Willis St, Wellington. AUCKLAND 1 Lioness by Emily Perkins (Bloomsbury, $25) Roarrrr! Perkins’ brilliant, award-winning, Marian-Keyes anointed, darkly funny, long ...22 hours ago
- Overturning Court Of Appeal Decision On Foreshore And Seabed Is Abuse Of Power
The 2004 Act vested ownership of the foreshore and seabed in the Crown, extinguishing any Māori claims to ownership and causing widespread outrage and protests among Māori communities. ...23 hours ago
- Gang crackdown: why anti-patch policies backfire – and what would actually work
Source: The Conversation (Au and NZ) – By Antje Deckert, Associate Professor (Criminology), Auckland University of Technology Getty Images Despite the connection between institutional harm and gang membership made clear in this week’s mammoth royal commission abuse-in care report, the government seems unlikely to soften its “get tough on ...23 hours ago
- Watch: Christopher Luxon's security cut short visit short ahead of protest
The prime minister was speaking to reporters during a walkabout with police in central Auckland. ...23 hours ago
- Overruling court on coastal rights risks new protests, Te Pāti Māori warns
Te Pāti Māori is warning a move to overturn a court decision risks a return of the big foreshore and seabed protests of 20 years ago. ...23 hours ago
- New Zealanders in action: When and who to watch in week one of the Paris Olympics
From Lewis Clareburt in the swimming to the start of the rowing – the first seven days of Paris 2024 promise to be big for New Zealand. There are few events that bring the country together quite like an Olympic Games. Nothing quite matches the excitement of getting up in ...23 hours ago
- The local science that just made a huge cameo in The Kardashians
Groundbreaking local science just showed up in the most surprising of places: the season finale of The Kardashians. In the season five finale of The Kardashians last night, several members of the family gathered together in one of their signature empty, cream-coloured rooms to hear test results that had been ...24 hours ago
- Can Israel and Hezbollah be pulled back from the brink of war?
Source: The Conversation (Au and NZ) – By Amin Saikal, Emeritus professor of Middle Eastern and Central Asian Studies, Australian National University The Middle East is on the brink of a possibly devastating regional war, with hostilities between Israel and Hezbollah reaching an extremely dangerous level. Washington has engaged in ...24 hours ago
- Lupus is more common and severe in Aboriginal and Torres Strait Islander peoples. Learning why is cr...
Source: The Conversation (Au and NZ) – By Laura Elizabeth Eades, Rheumatologist, Monash University Lupus is an inflammatory autoimmune illness, where the body’s immune system mistakenly attacks itself. Lupus can affect virtually any part of the body, although it most commonly affects the skin, joints and kidneys. The symptoms ...24 hours ago
- Government Fails To Recognise Parallels Between Whakapakari And Its Boot Camps
A law firm that specialises in working with survivors of abuse in State care is disappointed that the Government fails to recognise that its boot camps can be directly compared to previous boot camps from the 1990s and 2000s. ...1 day ago
- Crown breached Treaty principles in school reform – Waitangi Tribunal
A Waitangi Tribunal report has found the Crown breached Treaty principles in its review and reform of schools between 2018 and 2022. ...1 day ago
- Zero stars: Rating the experience of death and dying in Aotearoa
Dying is a natural part of life, like updating your Wof or seeing your hairdresser, but without the word-of-mouth recs that help guarantee a good service. What if we changed that? Dying Reviews received by The Spinoff have had the names of organisations redacted while Hospice NZ collects further data. ...1 day ago
- Not one, but two meteor showers are about to peak – here’s how to catch the stellar show
Source: The Conversation (Au and NZ) – By Jonti Horner, Professor (Astrophysics), University of Southern Queensland Mike Lewinski/Flickr, CC BY On any clear night, if you gaze skywards long enough, chances are you’ll see a meteor streaking through the sky. Some nights, however, are better than others. At ...1 day ago
- Ministry of Education puts 100 school building projects on ice
Deferring the builds and rescoping 110 others will save $2 billion, the ministry says. ...1 day ago
- How Tāmaki Makaurau became home to the world’s only lesbian museum
Despite having no bars or other designated spaces for lesbians, Auckland boasts a small but mighty lesbian museum. So how did it get here? The past 18 months has brought increasing hostility towards the queer community across Aotearoa. Kellie-Jay Keen-Minshull’s anti-trans rally in Tamaki Makaurau last March led to a ...1 day ago
- Protest At French Embassy Calls Out Hypocrisy In Kanaky As Paris Olympics Begin
Poneke Antifascist Coalition has invited Wellingtonians to stand in solidarity with the Kanak people at 12pm today outside the French Embassy in Wellington. ...1 day ago
- Chicken wire, AI and mobile phones on sticks: how the drone war in Ukraine is driving a fierce battl...
Source: The Conversation (Au and NZ) – By Peter Layton, Visiting Fellow, Strategic Studies, Griffith University Drones are the signature technology of the Ukraine war. A few miniature aircraft designs were used in the war’s early days, but an incredible array of drones have now evolved. There are different types, ...1 day ago
- What happens in my brain when I get a migraine? And what medications can I use to treat it?
Source: The Conversation (Au and NZ) – By Mark Slee, Associate Professor, Clinical Academic Neurologist, Flinders University Francisco Gonzelez/Unsplash Migraine is many things, but one thing it’s not is “just a headache”. “Migraine” comes from the Greek word “hemicrania”, referring to the common experience of migraine being predominantly ...1 day ago
- How old, inefficient housing and time-of-use electricity rates are leaving some households worse off
Source: The Conversation (Au and NZ) – By Lee White, Senior Lecturer and Horizon Fellow, School of Social and Political Sciences, University of Sydney Australia was slow to introduce minimum building standards for energy efficiency. The Nationwide House Energy Rating Scheme (NatHERS) only came into force in 2003. Older homes ...1 day ago
- Landmark new research shows how global warming is messing with our rainfall
Source: The Conversation (Au and NZ) – By Steven Sherwood, Professor of Atmospheric Sciences, Climate Change Research Centre, UNSW Sydney The past century of human-induced warming has increased rainfall variability over 75% of the Earth’s land area – particularly over Australia, Europe and eastern North America, new research shows. ...1 day ago
- Timber venues, river swimming and re-use: how the Paris Olympics is going green – and what it’s ...
Source: The Conversation (Au and NZ) – By Tony Heynen, Program Coordinator, Sustainable Energy, The University of Queensland A temporary stadium in the Champ-de-Mars, Paris Ekaterina Pokrovsky/Shutterstock As Paris prepares to host the Olympic and Paralympic Games, the sustainability of the event is coming under scrutiny. The organisers have promoted ...1 day ago
- An Ode to Newtown Sports Bar, Wellington’s last great pub
A night of karaoke and community in a pub that feels like a memory. You’d barely even notice it, unless you knew to look. Tucked away behind a liquor store on busy Constable Street is the capital’s last great pub. Newtown Sports Bar is an emblem of the pub culture ...1 day ago
- Health commissioner in meetings over new Dunedin Hospital cost blowout
The spotlight will then turn on the proposed new regional hospitals for Nelson, Hawke’s Bay, Tauranga and Palmerston North The post Health commissioner in meetings over new Dunedin Hospital cost blowout appeared first on Newsroom. ...1 day ago
- Declining PhD student numbers are a warning sign for NZ’s future knowledge economy
Source: The Conversation (Au and NZ) – By Ian Wright, Professor in Marine Geology, University of Canterbury Louise Corcoran/Getty Images The decline in the number of doctoral candidates at New Zealand universities is a worrying sign for the country’s effort to build a knowledge-based economy. Aotearoa New Zealand’s ...1 day ago
- Migrant workers have long been too scared to report employer misconduct. A new visa could change thi...
Source: The Conversation (Au and NZ) – By Laurie Berg, Associate Professor, University of Technology Sydney defotoberg/Shutterstock Migrant worker exploitation is entrenched in workplaces across Australia. Tragically, a deep fear of immigration consequences means most unlawful employer conduct goes unreported. On Wednesday, however, the government officially launched a ...1 day ago
- The chaotic history of the Olympics in Paris, where one games nearly ended the movement – and the ...
Source: The Conversation (Au and NZ) – By Vaughan Cruickshank, Senior Lecturer in Health and Physical Education, University of Tasmania Paris is about to host its third summer Olympics. While we don’t yet know what the legacy of this year’s games will be, let’s take the opportunity to reflect on ...1 day ago
- ‘Bloodbath’, ‘bullseye’, ‘America’s Hitler’: why has our political rhetoric gotten so ...
Source: The Conversation (Au and NZ) – By Hugh Breakey, Deputy Director, Institute for Ethics, Governance & Law, Griffith University In the wake of the assassination attempt on former US President Donald Trump, there were calls from both sides of US politics, as well as internationally, to reduce the brutal, ...1 day ago
- Politics, security and the Seine: where the Paris Olympics’ flashpoints will be
Source: The Conversation (Au and NZ) – By Keith Rathbone, Senior Lecturer, Modern European History and Sports History, Macquarie University Two high-profile assaults on Australians in Paris have raised concerns about security ahead of the Olympic Games. On Saturday evening, a young woman was allegedly sexually assaulted by a ...1 day ago
- Leaked Health NZ restructure proposal shines light on latest job cuts
There's "shock and dismay" at the health body with another "brutally fast" round of redundancies looming, one insider says. ...1 day ago
- Revisiting the cost of dying
Dying is inevitable and, so it seems, is it costing a lot, writes Stewart Sowman-Lund in today’s extract from The Bulletin. To receive The Bulletin in full each weekday, sign up here. The cost of dying ...1 day ago
- The state care decision that rippled through four generations
The government took Joyce Harris's first baby and sent her off to a girls' home. Half a century on - and out of oceans of hurt - it asked her to be a mother figure. ...1 day ago
- Mt Victoria Tunnel, Basin Reserve plans: NZTA spent seven times more on consultants than on its own ...
Staff working on a second Mt Victoria Tunnel and the Basin Reserve upgrade were paid $175,000 - but consultants were paid nearly $1.3 million. ...1 day ago
- Will Gen X ever be able to retire?
Caught between ageing parents and struggling kids, retirement planning is tough for a whole generation. ...1 day ago
- Minister defends lowered child poverty targets as 'achievable'
Louise Upston has rejected criticisms of lowered child poverty reduction targets, saying they are achievable and ambitious. ...1 day ago
- What is the wildest Brokenwood Mysteries death of all time?
It’s the deadliest fictional town in the country, but which death has been the most bonkers? Alex Casey looks back at 10 seasons of The Brokenwood Mysteries to find out. Warning: The following ranking story contains famous New Zealand actors appearing to be dead (not alive). The Spinoff has been ...1 day ago
- ‘It’s a no-brainer’: Why Aotearoa needs to ride the wave of water cremation
Water cremation is the biggest thing to happen to the death industry in the last 100 years. Alex Casey meets the people trying to bring it to Aotearoa. Through a set of mirrored doors down the industrial end of Christchurch’s St Asaph Street, death is getting a new lease on ...1 day ago
- This week’s bestselling books – July 26
NONFICTION 1 The Last Secret Agent by Pippa Latour & Jude Dobson (Allen & Unwin, $37.99) 2 The Life of Dai by Dai Henwood and Jaquie Brown (HarperCollins, $39.99) 3 A Life Less Punishing by Matt Heath (Allen & Unwin, $37.99) 4 Waitohu by Hinemoa Elder (Penguin Random House, $35) ...1 day ago
On re-read, there were quite a few other lessons that I missed. I will leave them for comments to elucidate.
But I will take the most obvious.
Long haul flights obviously need wider separation between passengers. That is pretty good separation. It wasn't enough if people were as masked as they said.
Eyeballing that separation, I'd definitely go for a window-seat if I couldn't get out of flying altogether. The aisle side looks a lot riskier, maybe due to bathroom walks by infected passengers? For extra safety you could have a depressurized plane filled with passengers all on independent individual oxygen supplies (scuba tanks is how I picture it, but probably ducted from central tanks). It'd be really cold and unpleasant though.
To be of much benefit, the 3day test really should be alongside managed isolation in the country of origin. Which I seem to recall Baker including in his initial recommendations, though don't have a source to hand. The logistics and enforcement of that would be a bit tricky though.
Problem is that I don't want to rely on managed isolation in the Ukraine or most of the other places this set of passengers came from.
I certainly wouldn't trust it from uncontrolled mayhem places like the US.
Probably the toilet would have the highest viral load on a long haul flight.
I would like to know if swabs are taken from the toilet area and tested?
Very interesting and a few links to follow up on.
Regarding the effects of vaccines on prevention or reduction of symptomatic disease (i.e. becoming sick) and prevention of spreading the infection, here’s a nice clarifying article on that:
https://www.stuff.co.nz/national/health/coronavirus/123886555/covid19-few-vaccines-prevent-infection–heres-why-thats-not-a-problem
In other words, we don’t know yet which kind of immunity we may enjoy. It could well be different with different vaccines.
Maybe it is wise to wait with rolling out vaccines in NZ 😉
Saw a RNZ report on a Otago epidemiologist (not Baker!) saying we may need to do more blockage at the border from places with out of control epidemics. Worried about how thin the border defenses are.
Problem is that is effectively everywhere in a few more months.
Looking at border staff vaccinations as a extra will help. But it is just another few percent protection rather than a panacea.
I would agree that inside the border has gotten really slack. Any case any outbreak inside will now need a wide set of lockdowns.
Yup, that was Prof. Nick Wilson.
I posted a comment earlier today about the new variant becoming the dominant one globally: https://thestandard.org.nz/open-mike-11-01-2021/#comment-1774115.
It does make sense to vaccinate frontline and border staff first.
I agree that New Zealand has become complacent and is relying too much on the frontline defence, which will be breached again at some stage, unfortunately; it is simply a numbers game and therefore a matter of time, i.e. not “if” but “when”.
When shit hits the fan, the blame games will start, again. Anyway, this is drifting away from your OP 😉
Probably it was on one news last night the reason for not opening up more MIQ facilities is because there is not the staff to manage the isolation/quarantine.
Not sure how popular to have a lock out before a lockdown for a limited period a month. This could be required as it is a not if but a when for a community out break.
Thanks for the link, Incognito.
Answered a few questions, but the answers largely fell into the 'We don't know yet' file. Not enough assurance for me to be pushing my way to the front of any queue.
Thank you for your response, which I find slightly puzzling.
I assume you’re not keen to be the first to be vaccinated for some reason. Although our Government has ensured purchase & supply of vaccines, it is not rushing to roll out any vaccination program yet. In other words, NZ is not first in the queue.
Why would you hesitate or delay? What “assurance” would change your mind, if I may ask?
Sure ask away.
What would I be vaccinated for? Which strain of Covid? Do I run the risks of passing that on to Mum? Plus I have a healthy disrespect for Big Pharma.
A bit like the annual flu jab, you get innoculated for last year's illness.
The massive rush that this medication has arrived with makes the inner cynic in me wary.
Another thread to the thinking is the false sense of security society has about the vaccine. Once we get the jab, everything will be alright, back to BAU.
One of the positive sides to this pandemic is folk learning halfway decent hand hygiene. Coming out of a lifetime of kitchen work it's great that others have caught up.
Edit, without telling Nana how to suck eggs, perhaps this is better on OM, we saw how quickly Mike Smith’s post on Julian Assange turned sour quick…
I’ll answer a few while I think about timers.
As far as I am aware most of the current released vaccines are targeting a particular attachment point (the bushy bits in a covid-19 virus) that it uses to attach to cells.
This current strains have vary limited variations in that area because that particular bit was how they managed to species jump to humans. So current vaccines should trigger the immune system to recognise that. So they should all work with varying levels of effectiveness.
It isn’t like the 1700 odd base pairs in a influenza variant that have virtually no error checking. This is a 32000 base pair virus with a lot of error checking. It mutates or recombines at a much lower rate. The only reason that we’re seeing any significant strains is because there were ancestral strains present at the outbreak in Wuhan, and then it had a very large number of hosts to play recombination games in.
Different type of disease.
With covid vaccines, the question is going to be different about effectiveness. It won’t be about coping with this years model like influenza. It will be how long the immune responses persist in humans. We won’t know that for years because we have to wait until the immune response stops either induced from vaccines or from ‘natural’ immunity after having it.
But Covid-19’s close cousin SARS had immune responses that have persisted for up to 15 years. On the other hand Covid common cold immunities seem to last for only a few years. The difference appears to be to do with how much of a immune response was triggered in the first place. The people getting SARS tended to get very sick very fast, which was why it was so easy to stamp out. Getting covid common cold just makes people a bit miserable.
So covid-19 vaccines need to trigger a strong response without making people sick. We won’t know how effective the first is for a while. The vaccine testing has mostly focused on how to make sure people didn’t get too sick.
It is one of the first diseases that came after we understood viruses, know how to produce vaccines for them (something that only really only started in the 1950s), and had a massive widespread economic impact that caused money to be thrown at it. It isn’t a stealthy retrovirus like HIV (which we still don’t have a vaccine for). It also helps when producing vaccines to have large numbers of test subjects – it abbreviates the testing process.
But many of the vaccines have been going through the usual semi-public government testing. I don’t have a problem with that. There will be unforeseen effects as it gets rolled out to wider populations because people aren’t exactly the same. There will be a lot of data collecting – same as for every vaccine.
Because we have the luxury of moderately effective border control – we can wait. But it is all about risk management. The first group that needs it are those at greatest risk of spreading – our border people and medical staff. After that the elderly who die from this too fast. etc etc…
I have a vaccine against people acting like non-listening arseholes. I just release my inner arrogant sarcastic arsehole, and then turn an amplifier up on it. This is one of my posts.
I have never had an issue with vaccination. When it comes to vaccination for Covid I would want to know what the side affects are for rare auto immune conditions where several per million are diagnosed with the condition annually. There would be no data on this as it would take years to accumulate.
I would agree. We aren’t going to have as much information on these vaccines as we would normally have.
If someone has conditions that could be an issue, then there has to be a tradeoff on risk.
But that is always the case with vaccines or medicines. This one is just collapsed into a shorter time frame.
The question is going to be if you take a vaccine with a possible unknown risk against any particular medical conditions. Or get a possibky fatal disease that may have long term consequences. Or constrain your life to minimize risk of infection. There are no absolute certainties.
About the only certainty is that after the distribution of vaccines gets widespread, at some point the government and other citizens will start reducing the barriers to infection.
Thanks for yr considered response lprent.
As you point out, here in NZ we have the luxury of time and distance.
Ta
An interesting article but it still leaves unanswered questions about the method of transmission, especially given the negative tests shown – from the last figure 26C is the luckiest I would say, assuming light blue is the original case (A).
I am not sure " In particular the pattern in row 24 with the two people not getting a positive result is pretty abnormal." is necessarily correct though. If F and G were newly infected on the flight, they were themselves not likely to have been infectious during the flight. The last figure and the article text show that G caught coronavirus from their travel partner subsequent to the flight.
It is possible that the people who were infected on the flight caught it by using the same toilet as the original case. I can well imagine that someone who is sick will relax their hygiene in an area where they can't be seen. If we discount cases B and G as having caught coronavirus on the flight, then 4 people did. From the seating plan, that's just under a 1 in 20 chance of catching it for those in the vicinity of case A, so how likely is it that there were a lot of infectious droplets in the air?
The main form of transmission for covid-19 appears to be from short distance airborne droplets, with a subsidiary and lesser transmission from some surfaces. This seems to be pretty clear with this flight – implies short distance droplets. The distance between infected and infectious is very low and entirely in aisles.
If the passengers A and B were the infectious primary source, then they managed to infect C, D, E, and F in flight. Presumably F then infected G in quarantine.
But as the seating diagram indicates, there are 9 people (including G) who were within similar droplet distances who didn't get directly infected during the flight according to subsequent tests.
Since 4 did, that means a 4/13 probability of being infected at close range.
The probability looks very high in aisles – 4/7.
I presume that your 1/20 ratio is based on 4/87 – ie all passengers less A and B. But there has been little to no evidence anywhere of longer range infection past about 3 metres except for some rare cases of contact or enclosed spaces that don't clear the air – like lifts. If the environmental systems were a problem – then you'd expect a much wider spread issue.
Presumably surface contact or residual droplets in the toilet would have had a similar probability for a lot more passengers than those we have a seating plan for. A lot of a passengers will use toilets in a plane – they always seem to have a queue on long haul.
Pity that they obviously didn't have camera footage. I suspect that the pattern and frequency of contacts would have been enlightening. Like when and which toilets were accessed and who was seated and masked at the time. But my bet is that getting up and moving to toilets or stretching would be the theory to disprove. Droplets travel further when emitted at height.
The main form of transmission may be short distance airborne droplets, but that doesn't rule out fomite transmission. I think that in this case fomite transmission (probably from the toilet) is the most likely cause. With the plane mostly empty there would have been a smaller intersection of possible infection candidates.
How would the virus be internalised then? It doesn’t go through the skin so it could only happen by touching mouth, nose, or eyes with contaminated hands/fingers. I guess it is entirely possible that the ‘lucky’ ones had much better habits in the sense of not touching their faces.
Yes travel to see our son… a long way off for all the reasons raised. There are still more questions than answers.
I do think we should be praising and paying a premium to those doing the job of keeping us safe. I read many criticisms, yet our managed isolation is working.
We need to train more staff, give real down time and rest for those charged with the task, so fatigue is not a cause of mismanagement, also a bonus could be paid if an isolation facility is rated safe and secure each calendar month. Carrot and stick.
Perhaps in the end a certificate of vaccination/inoculation to travel will be needed, as some diseases have been managed previously.
Let us hope we manage this infection as Queensland did, quickly reacting to an incursion of the new variant, until vaccination and herd immunity is achieved, which is some way off yet.
That also assumes these vaccines will control the infection? That is the $64000 ? Only time will tell…so waiting…..
Yep. Some of the botched distribution in the US and probably in the UK should be public enough to shed light on how not to do it. The US hopefully will soon lose theire major bullshit factor.
Europe should provide a better controlled test for how to do it better.
China has too few cases at present to get any good idea even if they didn't do the idiotic propaganda that they seem to be focused on.
When India gets underway, that should be pretty clear. Some of the biggest vaccine manufacturing gets done there. The shortened distance between provider and recipients has proved effective in previous vaccine rollouts fro correcting problems.
Russia will be interesting. While they have a wide public health system, it doesn't seem to be even and appears to have political aspects that aren't usually helpful at being effective. The early phases of covid there were perfect, all ok , and then a Brazil or US like high.