 Plan B activists still think NZ should be like Sweden
Plan B activists still think NZ should be like Sweden
Written By:
- Date published:
11:50 am, December 26th, 2020 - 171 comments
Categories: boris johnson, covid-19, health, making shit up, spin, uncategorized, you couldn't make this shit up -
Tags:
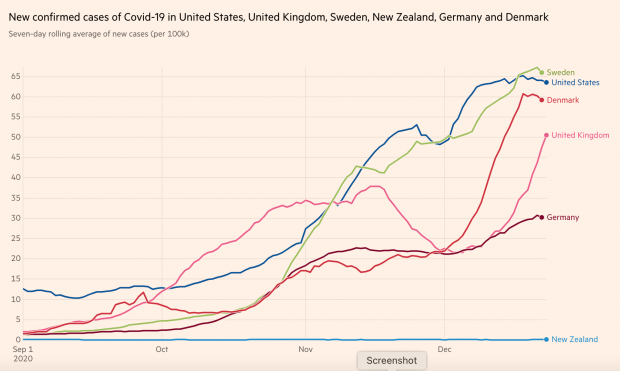
There is a new strain of Covid 19 recently discovered in the UK that is considerably more infectious than the originally discovered strain.
From the ABC:
A new variant of SARS-CoV-2, the virus which causes COVID-19, is thought to be driving increased transmission of the disease in parts of the UK.
The government has placed some regions including London under new, stricter coronavirus restrictions, known as Tier 4. People in Tier 4 areas will not be able to gather with anyone outside their household for Christmas, while those in the rest of the country can only gather on Christmas Day itself.
British Prime Minister Boris Johnson and his chief scientific advisors said that the new variant could increase transmission of COVID-19 by as much as 70 per cent and increase the R or reproduction number by 0.4 per cent.
The discovery has caused Boris Johnson to severely curtail Christmas celebrations in the UK, something that you can bet was the last thing that he wanted to do.
The Observer in an editorial published in the Guardian puts it in these terms:
‘We don’t want to cancel Christmas… I think that would be inhuman,” the prime minister said just last Wednesday in response to calls from scientific experts to reduce the relaxation of social restrictions allowing households to mix over Christmas.
Four days later, he was forced to abruptly change course in light of alarming data indicating a steep increase in infection rates in London and parts of the south-east and east of England, thought to be linked to a new and more easily transmitted variant of Covid-19. The government was right to immediately impose tougher tier 4 restrictions on these parts of the country and elsewhere to restrict indoors household mixing to Christmas Day only.
It is clear that without these measures there would have been a huge risk of a rise in infection and death rates in January and February as a result of intergenerational mixing over Christmas, particularly endangering older people and those with pre-existing health conditions. This is likely to have put the NHS under intolerable strain as it reached the worst point of the year in terms of winter pressures, compromising the treatment not only of people with severe Covid symptoms, but with any serious health condition. The fact that vaccines are being rolled out to high-priority groups, with more comprehensive coverage months away, underlines how ill-judged it would be to trigger a larger-than-necessary spike in the death rate with the end of this period of social restrictions in sight.
But the late nature of this decision will cause considerable pain and heartbreak to families who have been encouraged to look forward to Christmas for weeks by a prime minister who, in characteristic form, foolishly over-promised in an attempt to avoid being the bearer of bad news.
For weeks, scientific experts, including members of Sage, have urged caution with respect to Christmas relaxations, given the direction in which infection rates were heading. For weeks, they have warned that it is a question of balance and that relaxing restrictions against a backdrop of rising infection rates could lead to a significant number of avoidable deaths. It is understandable that the government wanted to allow people to see their families at Christmas after the year we have had. But Johnson should have been honest with the public that there was no guarantee of any Christmas relaxation, that it was contingent on the state of the play with the virus. Instead, he gave false reassurances and encouraged families to make and look forward to plans that, for many, will now not come to pass.
Meanwhile here in Aotearoa New Zealand we are celebrating Christmas, going to the beach, going shopping or to the cricket and generally doing what we have yearned to do all year.
Makes you want to heap praise on the Government for its go hard and go early strategy?
Not for everyone.
So how does a ginger group that so far has never budged from the thought that Sweden may be better respond? By criticising the policy that has without any doubt resulted in our rather welcome position. Because as the rest of the world struggles handling this evil virus for now at least we can live relatively normal lives.
Plan B academics have written a letter to the editor that has been published in the Royal New Zealand College of Medical Practitioners claiming that chasing elimination through lockdowns is stamping out livelihoods and lives.
Short version of the letter:
- Aotearoa New Zealand has an elimination strategy.
- There is no successful vaccine which will take at least four years and may be a decade away.
- Tourism, our biggest export earner, will remain a casualty and the domestic economy will endure ongoing disruption.
- The WHO believes that lock downs are not a long term solution for the virus.
- Health and the economy are inseparable and the single most important determinant of health is income.
- Because the economy has retracted a reduction in life expectancy can be expected.
- New Zealand has maintained its elimination strategy despite the WHO and most countries deciding to adapt rather than eliminate.
- “Hard lockdowns are still the tool our government plans to reach for to ‘stamp out the virus’”.
The letter concludes with this call to arms:
How many more lockdowns, billions of dollars and social and health harm is an acceptable price to pay before this misguided and expensive strategy is abandoned? We implore Prime Minister Jacinda Ardern, Director-General of Health Dr Ashley Bloomfield, and fellow health advisors to reflect on the points raised in this paper and to abandon elimination as a strategy and the use of lockdowns. We believe that future policy should return to the initial approach that was taken. That is to reduce transmission of COVID-19 through reasonable use of infection control, to maintain capacity in our hospitals and intensive care, while focusing public health and infection control efforts to protect the frail and elderly of our community.
There is quite a bit to unpick in this letter, mainly how can a bunch of academics get things so wrong? For instance:
- It is correct that we do have an elimination strategy.
- There are two vaccines being rolled out right now and others in the pipeline. Big Pharma has thrown a lot of effort and resources into developing a vaccine as quickly as possible.
- Sure international tourism has tanked but domestic tourism has picked up. The economy is adjusting.
- The WHO Director General Tedros Adhanom Ghebreyesus has listed New Zealand among the countries that have done well during the pandemic.
- This reads like something the Taxpayers Union would say.
- Annual GDP grew 0.4% and the latest quarter’s growth was 14%, a remarkable result that is among the best in the world. Going hard and going early and then allowing society to reopen worked pretty well.
- Most countries have decided to adapt because they have no choice. They all wish they were New Zealand right now.
- The Government has shown an increasingly sophisticated response to the virus with the second “lockdown” being far more permissive and targeted than the first and with other examples of community spread being dealt with by way of contact tracing and advanced genomic analysis which can pinpoint where the virus may have come from.
I mean, really?
Professor of Health Michael Baker has also poured scorn on the content of the letter. From the Herald:
… University of Otago professor of public health Michael Baker told the Herald the letter was almost unfit for publication due to its inaccuracy and, in his opinion the authors were living in an alternate reality.
“I assume that article couldn’t have been peer-reviewed, really, because it’s got things in it which are patently absurd,” Baker said.
“I don’t know what they’re basing their claims on. I mean just to begin with, as soon as you say ‘There is no hope of a vaccine’, and they pretty much say that, or ‘It’s very unlikely’, when the world seems to be awash with fantastic vaccine candidates. I mean, surely you begin to doubt the credibility of the entire argument.”
In the letter, the Plan B group claim “a vaccine may never eventuate. After 37 years and billions of dollars invested, an HIV vaccine remains elusive”.
Baker also criticised the logic of the Plan B group’s focus on the economic impact of lockdowns, saying you needed to judge that cost in the context of all other alternatives.
“What economists always say is, it’s not about whether something costs a lot of money or not. It’s whether there is a better alternative that will give you a better result and cost less,” Baker said.
“If you haven’t got that alternative you’re better to stick with Plan A, rather than shoot off to this planet B which appears to have a completely alternate logic structure to it.
“That’s what I find almost scandalous, that university academics are putting out material that is so poorly argued and is cherry-picking evidence in a very selective way and doesn’t make any sense.”
By all means let’s have a reasoned debate about what the best response is and how we should be adapting and changing our approach to the virus. But when we have this debate ginger groups should at least try to ensure that their basic understanding of things is sound.
171 comments on “Plan B activists still think NZ should be like Sweden ”
- Comments are now closed
- Comments are now closed
Recent Comments
- Bernard’s Saturday Soliloquy for the week to July 27
 Photo: Lynn Grieveson / The KākāTL;DR: My top six things to note around housing, climate and poverty in Aotearoa’s political economy in the week to July 27 were:1. The Minister for Ford Rangers strikes againTransport Minister Simeon Brown was again the busiest of the Cabinet ministers this week, announcing an ...34 mins ago
Photo: Lynn Grieveson / The KākāTL;DR: My top six things to note around housing, climate and poverty in Aotearoa’s political economy in the week to July 27 were:1. The Minister for Ford Rangers strikes againTransport Minister Simeon Brown was again the busiest of the Cabinet ministers this week, announcing an ...34 mins ago - Ticket To Anywhere
 You got a fast carAnd I want a ticket to anywhereMaybe we make a dealMaybe together we can get somewhereAny place is betterYesterday’s newsletter, Trust In Me, on the report of abuse in state care, and by religious organisations, between 1950 and 2019, coupled with the hypocrisy of Christopher Luxon ...1 hour ago
You got a fast carAnd I want a ticket to anywhereMaybe we make a dealMaybe together we can get somewhereAny place is betterYesterday’s newsletter, Trust In Me, on the report of abuse in state care, and by religious organisations, between 1950 and 2019, coupled with the hypocrisy of Christopher Luxon ...1 hour ago - Stories of varying weight
 6 hours ago
6 hours ago - Balancing External Security and the Economy
 New Zealand is again having to reconcile conflicting pressures from its military and its trade interests. Should we join Pillar Two of AUKUS and risk compromising our markets in China? For a century after New Zealand was founded in 1840, its external security arrangements and external economics arrangements were aligned. ...18 hours ago
New Zealand is again having to reconcile conflicting pressures from its military and its trade interests. Should we join Pillar Two of AUKUS and risk compromising our markets in China? For a century after New Zealand was founded in 1840, its external security arrangements and external economics arrangements were aligned. ...18 hours ago - Weekly Climate Wrap: The unravelling of the offsets
23 hours ago
- What makes us tick
 This morning the sky was bright.The birds, in their usual joyous bliss. Nature doesn’t seem to feel the heat of what might angst humans.Their calls are clear and beautiful.Just some random thoughts:MāoriPaul Goldsmith has announced his government will roll back the judiciary’s rulings on Māori Customary Marine Title, which recognises ...1 day ago
This morning the sky was bright.The birds, in their usual joyous bliss. Nature doesn’t seem to feel the heat of what might angst humans.Their calls are clear and beautiful.Just some random thoughts:MāoriPaul Goldsmith has announced his government will roll back the judiciary’s rulings on Māori Customary Marine Title, which recognises ...1 day ago - Foreshore and seabed 2.0
 In 2003, the Court of Appeal delivered its decision in Ngati Apa v Attorney-General, ruling that Māori customary title over the foreshore and seabed had not been universally extinguished, and that the Māori Land Court could determine claims and confirm title if the facts supported it. This kicked off the ...1 day ago
In 2003, the Court of Appeal delivered its decision in Ngati Apa v Attorney-General, ruling that Māori customary title over the foreshore and seabed had not been universally extinguished, and that the Māori Land Court could determine claims and confirm title if the facts supported it. This kicked off the ...1 day ago - Gordon Campbell on the Royal Commission report into abuse in care
 Earlier this week at Parliament, Labour leader Chris Hipkins was applauded for saying that the response to the final report of the Royal Commission of Inquiry into Abuse in Care had to be “bigger than politics.” True, but the fine words, apologies and “we hear you” messages will soon ring ...1 day ago
Earlier this week at Parliament, Labour leader Chris Hipkins was applauded for saying that the response to the final report of the Royal Commission of Inquiry into Abuse in Care had to be “bigger than politics.” True, but the fine words, apologies and “we hear you” messages will soon ring ...1 day ago - The Kākā’s Pick 'n' Mix for Friday, July 26
 TL;DR: In news breaking this morning:The Ministry of Education is cutting $2 billion from its school building programme so the National-ACT-NZ First Coalition Government has enough money to deliver tax cuts; The Government has quietly lowered its child poverty reduction targets to make them easier to achieve;Te Whatu Ora-Health NZ’s ...1 day ago
TL;DR: In news breaking this morning:The Ministry of Education is cutting $2 billion from its school building programme so the National-ACT-NZ First Coalition Government has enough money to deliver tax cuts; The Government has quietly lowered its child poverty reduction targets to make them easier to achieve;Te Whatu Ora-Health NZ’s ...1 day ago - Weekly Roundup 26-July-2024
 Kia ora. These are some stories that caught our eye this week – as always, feel free to share yours in the comments. Our header image this week (via Eke Panuku) shows the planned upgrade for the Karanga Plaza Tidal Swimming Steps. The week in Greater Auckland On ...1 day ago
Kia ora. These are some stories that caught our eye this week – as always, feel free to share yours in the comments. Our header image this week (via Eke Panuku) shows the planned upgrade for the Karanga Plaza Tidal Swimming Steps. The week in Greater Auckland On ...1 day ago - God what a relief
 1 day ago
1 day ago - Trust In Me
 Trust in me in all you doHave the faith I have in youLove will see us through, if only you trust in meWhy don't you, you trust me?In a week that saw the release of the 3,000 page Abuse in Care report Christopher Luxon was being asked about Boot Camps. ...1 day ago
Trust in me in all you doHave the faith I have in youLove will see us through, if only you trust in meWhy don't you, you trust me?In a week that saw the release of the 3,000 page Abuse in Care report Christopher Luxon was being asked about Boot Camps. ...1 day ago - The Hoon around the week to July 26
TL;DR: The podcast above of the weekly ‘hoon’ webinar for paying subscribers last night features co-hosts and talking about the Royal Commission Inquiry into Abuse in Care report released this week, and with:The Kākā’s climate correspondent on a UN push to not recognise carbon offset markets and ...1 day ago
- The Kākā’s Journal of Record for Friday, July 26
 TL;DR: As of 6:00 am on Friday, July 26, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:Transport: Simeon Brown announced $802.9 million in funding for 18 new trains on the Wairarapa and Manawatū rail lines, which ...1 day ago
TL;DR: As of 6:00 am on Friday, July 26, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:Transport: Simeon Brown announced $802.9 million in funding for 18 new trains on the Wairarapa and Manawatū rail lines, which ...1 day ago - Radical law changes needed to build road
The northern expressway extension from Warkworth to Whangarei is likely to require radical changes to legislation if it is going to be built within the foreseeable future. The Government’s powers to purchase land, the planning process and current restrictions on road tolling are all going to need to be changed ...1 day ago
- Skeptical Science New Research for Week #30 2024
 Open access notables Could an extremely cold central European winter such as 1963 happen again despite climate change?, Sippel et al., Weather and Climate Dynamics: Here, we first show based on multiple attribution methods that a winter of similar circulation conditions to 1963 would still lead to an extreme seasonal ...2 days ago
Open access notables Could an extremely cold central European winter such as 1963 happen again despite climate change?, Sippel et al., Weather and Climate Dynamics: Here, we first show based on multiple attribution methods that a winter of similar circulation conditions to 1963 would still lead to an extreme seasonal ...2 days ago - First they came for the Māori
 2 days ago
2 days ago - Join us for the weekly Hoon on YouTube Live
 Photo by Joshua J. Cotten on UnsplashWe’re back again after our mid-winter break. We’re still with the ‘new’ day of the week (Thursday rather than Friday) when we have our ‘hoon’ webinar with paying subscribers to The Kākā for an hour at 5 pm.Jump on this link on YouTube Livestream ...2 days ago
Photo by Joshua J. Cotten on UnsplashWe’re back again after our mid-winter break. We’re still with the ‘new’ day of the week (Thursday rather than Friday) when we have our ‘hoon’ webinar with paying subscribers to The Kākā for an hour at 5 pm.Jump on this link on YouTube Livestream ...2 days ago - Will the real PM Luxon please stand up?
 2 days ago
2 days ago - Will debt reduction trump abuse in care redress?
 Luxon speaks in Parliament yesterday about the Abuse in Care report. Photo: Hagen Hopkins/Getty ImagesTL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy today are:PM Christopher Luxon said yesterday in tabling the Abuse in Care report in Parliament he wanted to ‘do the ...2 days ago
Luxon speaks in Parliament yesterday about the Abuse in Care report. Photo: Hagen Hopkins/Getty ImagesTL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy today are:PM Christopher Luxon said yesterday in tabling the Abuse in Care report in Parliament he wanted to ‘do the ...2 days ago - Olywhites and Time Bandits
 About a decade ago I worked with a bloke called Steve. He was the grizzled veteran coder, a few years older than me, who knew where the bodies were buried - code wise. Despite his best efforts to be approachable and friendly he could be kind of gruff, through to ...2 days ago
About a decade ago I worked with a bloke called Steve. He was the grizzled veteran coder, a few years older than me, who knew where the bodies were buried - code wise. Despite his best efforts to be approachable and friendly he could be kind of gruff, through to ...2 days ago - Why were the 1930s so hot in North America?
This is a re-post from Yale Climate Connections by Jeff Masters and Bob Henson Those who’ve trawled social media during heat waves have likely encountered a tidbit frequently used to brush aside human-caused climate change: Many U.S. states and cities had their single hottest temperature on record during the 1930s, setting incredible heat marks ...2 days ago
- Throwback Thursday – Thinking about Expressways
Some of the recent announcements from the government have reminded us of posts we’ve written in the past. Here’s one from early 2020. There were plenty of reactions to the government’s infrastructure announcement a few weeks ago which saw them fund a bunch of big roading projects. One of ...2 days ago
- The Kākā’s Pick 'n' Mix for Thursday, July 25
 TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 7:00 am on Thursday, July 25 are:News: Why Electric Kiwi is closing to new customers - and why it matters RNZ’s Susan EdmundsScoop: Government drops ...2 days ago
TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 7:00 am on Thursday, July 25 are:News: Why Electric Kiwi is closing to new customers - and why it matters RNZ’s Susan EdmundsScoop: Government drops ...2 days ago - The Possum: Demon or Friend?
 Hi,I felt a small wet tongue snaking through one of the holes in my Crocs. It explored my big toe, darting down one side, then the other. “He’s looking for some toe cheese,” said the woman next to me, words that still haunt me to this day.Growing up in New ...2 days ago
Hi,I felt a small wet tongue snaking through one of the holes in my Crocs. It explored my big toe, darting down one side, then the other. “He’s looking for some toe cheese,” said the woman next to me, words that still haunt me to this day.Growing up in New ...2 days ago - Not a story
 Yesterday I happily quoted the Prime Minister without fact-checking him and sure enough, it turns out his numbers were all to hell. It’s not four kg of Royal Commission report, it’s fourteen.My friend and one-time colleague-in-comms Hazel Phillips gently alerted me to my error almost as soon as I’d hit ...2 days ago
Yesterday I happily quoted the Prime Minister without fact-checking him and sure enough, it turns out his numbers were all to hell. It’s not four kg of Royal Commission report, it’s fourteen.My friend and one-time colleague-in-comms Hazel Phillips gently alerted me to my error almost as soon as I’d hit ...2 days ago - The Kākā’s Journal of Record for Thursday, July 25
 TL;DR: As of 6:00 am on Thursday, July 25, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day were:The Abuse in Care Royal Commission of Inquiry published its final report yesterday.PM Christopher Luxon and The Minister responsible for ...2 days ago
TL;DR: As of 6:00 am on Thursday, July 25, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day were:The Abuse in Care Royal Commission of Inquiry published its final report yesterday.PM Christopher Luxon and The Minister responsible for ...2 days ago - A tougher line on “proactive release”?
The Official Information Act has always been a battle between requesters seeking information, and governments seeking to control it. Information is power, so Ministers and government agencies want to manage what is released and when, for their own convenience, and legality and democracy be damned. Their most recent tactic for ...3 days ago
- 'Let's build a motorway costing $100 million per km, before emissions costs'
 TL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy today are:Transport and Energy Minister Simeon Brown is accelerating plans to spend at least $10 billion through Public Private Partnerships (PPPs) to extend State Highway One as a four-lane ‘Expressway’ from Warkworth to Whangarei ...3 days ago
TL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy today are:Transport and Energy Minister Simeon Brown is accelerating plans to spend at least $10 billion through Public Private Partnerships (PPPs) to extend State Highway One as a four-lane ‘Expressway’ from Warkworth to Whangarei ...3 days ago - Lester's Prescription – Positive Bleeding.
 I live my life (woo-ooh-ooh)With no control in my destinyYea-yeah, yea-yeah (woo-ooh-ooh)I can bleed when I want to bleedSo come on, come on (woo-ooh-ooh)You can bleed when you want to bleedYea-yeah, come on (woo-ooh-ooh)Everybody bleed when they want to bleedCome on and bleedGovernments face tough challenges. Selling unpopular decisions to ...3 days ago
I live my life (woo-ooh-ooh)With no control in my destinyYea-yeah, yea-yeah (woo-ooh-ooh)I can bleed when I want to bleedSo come on, come on (woo-ooh-ooh)You can bleed when you want to bleedYea-yeah, come on (woo-ooh-ooh)Everybody bleed when they want to bleedCome on and bleedGovernments face tough challenges. Selling unpopular decisions to ...3 days ago - Casey Costello gaslights Labour in the House
Please note:To skip directly to the- parliamentary footage in the video, scroll to 1:21 To skip to audio please click on the headphone icon on the left hand side of the screenThis video / audio section is under development. ...3 days ago
- Why is the Texas grid in such bad shape?
This is a re-post from the Climate Brink by Andrew Dessler Headline from 2021 The Texas grid, run by ERCOT, has had a rough few years. In 2021, winter storm Uri blacked out much of the state for several days. About a week ago, Hurricane Beryl knocked out ...3 days ago
- Gordon Campbell on a textbook case of spending waste by the Luxon government
Given the crackdown on wasteful government spending, it behooves me to point to a high profile example of spending by the Luxon government that looks like a big, fat waste of time and money. I’m talking about the deployment of NZDF personnel to support the US-led coalition in the Red ...3 days ago
- The Kākā’s Pick 'n' Mix for Wednesday, July 24
 TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 7:40 am on Wednesday, July 24 are:Deep Dive: Chipping away at the housing crisis, including my comments RNZ/Newsroom’s The DetailNews: Government softens on asset sales, ...3 days ago
TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 7:40 am on Wednesday, July 24 are:Deep Dive: Chipping away at the housing crisis, including my comments RNZ/Newsroom’s The DetailNews: Government softens on asset sales, ...3 days ago - LXR Takaanini
As I reported about the city centre, Auckland’s rail network is also going through a difficult and disruptive period which is rapidly approaching a culmination, this will result in a significant upgrade to the whole network. Hallelujah. Also like the city centre this is an upgrade predicated on the City ...3 days ago
- Four kilograms of pain
 Today, a 4 kilogram report will be delivered to Parliament. We know this is what the report of the Royal Commission of Inquiry into Abuse in State and Faith-based Care weighs, because our Prime Minister told us so.Some reporter had blindsided him by asking a question about something done by ...3 days ago
Today, a 4 kilogram report will be delivered to Parliament. We know this is what the report of the Royal Commission of Inquiry into Abuse in State and Faith-based Care weighs, because our Prime Minister told us so.Some reporter had blindsided him by asking a question about something done by ...3 days ago - The Kākā’s Journal of Record for Wednesday, July 24
 TL;DR: As of 7:00 am on Wednesday, July 24, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:Beehive: Transport Minister Simeon Brown announced plans to use PPPs to fund, build and run a four-lane expressway between Auckland ...3 days ago
TL;DR: As of 7:00 am on Wednesday, July 24, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:Beehive: Transport Minister Simeon Brown announced plans to use PPPs to fund, build and run a four-lane expressway between Auckland ...3 days ago - Luxon gets caught out
NewstalkZB host Mike Hosking, who can usually be relied on to give Prime Minister Christopher Luxon an easy run, did not do so yesterday when he interviewed him about the HealthNZ deficit. Luxon is trying to use a deficit reported last year by HealthNZ as yet another example of the ...3 days ago
- A worrying sign
Back in January a StatsNZ employee gave a speech at Rātana on behalf of tangata whenua in which he insulted and criticised the government. The speech clearly violated the principle of a neutral public service, and StatsNZ started an investigation. Part of that was getting an external consultant to examine ...4 days ago
- Are we fine with 47.9% home-ownership by 2048?
 Renting for life: Shared ownership initiatives are unlikely to slow the slide in home ownership by much. Photo: Lynn Grieveson / The KākāTL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy today are:A Deloitte report for Westpac has projected Aotearoa’s home-ownership rate will ...4 days ago
Renting for life: Shared ownership initiatives are unlikely to slow the slide in home ownership by much. Photo: Lynn Grieveson / The KākāTL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy today are:A Deloitte report for Westpac has projected Aotearoa’s home-ownership rate will ...4 days ago - Let's Win This
 You're broken down and tiredOf living life on a merry go roundAnd you can't find the fighterBut I see it in you so we gonna walk it outAnd move mountainsWe gonna walk it outAnd move mountainsAnd I'll rise upI'll rise like the dayI'll rise upI'll rise unafraidI'll rise upAnd I'll ...4 days ago
You're broken down and tiredOf living life on a merry go roundAnd you can't find the fighterBut I see it in you so we gonna walk it outAnd move mountainsWe gonna walk it outAnd move mountainsAnd I'll rise upI'll rise like the dayI'll rise upI'll rise unafraidI'll rise upAnd I'll ...4 days ago - Waimahara: The Singing Spirit of Water
There’s been a change in Myers Park. Down the steps from St. Kevin’s Arcade, past the grassy slopes, the children’s playground, the benches and that goat statue, there has been a transformation. The underpass for Mayoral Drive has gone from a barren, grey, concrete tunnel, to a place that thrums ...4 days ago
- A major milestone: Global climate pollution may have just peaked
This is a re-post from Yale Climate Connections Global society may have finally slammed on the brakes for climate-warming pollution released by human fossil fuel combustion. According to the Carbon Monitor Project, the total global climate pollution released between February and May 2024 declined slightly from the amount released during the same ...4 days ago
- The Kākā’s Pick 'n' Mix for Tuesday, July 23
 TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 7:00 am on Tuesday, July 23 are:Deep Dive: Penlink: where tolling rhetoric meets reality BusinessDesk-$$$’s Oliver LewisScoop: Te Pūkenga plans for regional polytechs leak out ...4 days ago
TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 7:00 am on Tuesday, July 23 are:Deep Dive: Penlink: where tolling rhetoric meets reality BusinessDesk-$$$’s Oliver LewisScoop: Te Pūkenga plans for regional polytechs leak out ...4 days ago - The Kākā’s Journal of Record for Tuesday, July 23
 TL;DR: As of 6:00 am on Tuesday, July 23, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:Health: Shane Reti announced the Board of Te Whatu Ora- Health New Zealand was being replaced with Commissioner Lester Levy ...4 days ago
TL;DR: As of 6:00 am on Tuesday, July 23, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:Health: Shane Reti announced the Board of Te Whatu Ora- Health New Zealand was being replaced with Commissioner Lester Levy ...4 days ago - HealthNZ and Luxon at cross purposes over budget blowout
Health NZ warned the Government at the end of March that it was running over Budget. But the reasons it gave were very different to those offered by the Prime Minister yesterday. Prime Minister Christopher Luxon blamed the “botched merger” of the 20 District Health Boards (DHBs) to create Health ...4 days ago
- 2500-3000 more healthcare staff expected to be fired, as Shane Reti blames Labour for a budget defic...
 Long ReadKey Summary: Although National increased the health budget by $1.4 billion in May, they used an old funding model to project health system costs, and never bothered to update their pre-election numbers. They were told during the Health Select Committees earlier in the year their budget amount was deficient, ...4 days ago
Long ReadKey Summary: Although National increased the health budget by $1.4 billion in May, they used an old funding model to project health system costs, and never bothered to update their pre-election numbers. They were told during the Health Select Committees earlier in the year their budget amount was deficient, ...4 days ago - Might Kamala Harris be about to get a 'stardust' moment like Jacinda Ardern?
 As a momentous, historic weekend in US politics unfolded, analysts and commentators grasped for precedents and comparisons to help explain the significance and power of the choice Joe Biden had made. The 46th president had swept the Democratic party’s primaries but just over 100 days from the election had chosen ...5 days ago
As a momentous, historic weekend in US politics unfolded, analysts and commentators grasped for precedents and comparisons to help explain the significance and power of the choice Joe Biden had made. The 46th president had swept the Democratic party’s primaries but just over 100 days from the election had chosen ...5 days ago - Solutions Interview: Steven Hail on MMT & ecological economics
TL;DR: I’m casting around for new ideas and ways of thinking about Aotearoa’s political economy to find a few solutions to our cascading and self-reinforcing housing, poverty and climate crises.Associate Professor runs an online masters degree in the economics of sustainability at Torrens University in Australia and is organising ...5 days ago
- Reported back
The Finance and Expenditure Committee has reported back on National's Local Government (Water Services Preliminary Arrangements) Bill. The bill sets up water for privatisation, and was introduced under urgency, then rammed through select committee with no time even for local councils to make a proper submission. Naturally, national's select committee ...5 days ago
- Vandrad the Viking, Christopher Coombes, and Literary Archaeology
 Some years ago, I bought a book at Dunedin’s Regent Booksale for $1.50. As one does. Vandrad the Viking (1898), by J. Storer Clouston, is an obscure book these days – I cannot find a proper online review – but soon it was sitting on my shelf, gathering dust alongside ...5 days ago
Some years ago, I bought a book at Dunedin’s Regent Booksale for $1.50. As one does. Vandrad the Viking (1898), by J. Storer Clouston, is an obscure book these days – I cannot find a proper online review – but soon it was sitting on my shelf, gathering dust alongside ...5 days ago - Gordon Campbell On The Biden Withdrawal
History is not on the side of the centre-left, when Democratic presidents fall behind in the polls and choose not to run for re-election. On both previous occasions in the past 75 years (Harry Truman in 1952, Lyndon Johnson in 1968) the Democrats proceeded to then lose the White House ...5 days ago
- Joe Biden's withdrawal puts the spotlight back on Kamala and the USA's complicated relatio...
 This is a free articleCoverageThis morning, US President Joe Biden announced his withdrawal from the Presidential race. And that is genuinely newsworthy. Thanks for your service, President Biden, and all the best to you and yours.However, the media in New Zealand, particularly the 1News nightly bulletin, has been breathlessly covering ...5 days ago
This is a free articleCoverageThis morning, US President Joe Biden announced his withdrawal from the Presidential race. And that is genuinely newsworthy. Thanks for your service, President Biden, and all the best to you and yours.However, the media in New Zealand, particularly the 1News nightly bulletin, has been breathlessly covering ...5 days ago - Why we have to challenge our national fiscal assumptions
 A homeless person’s camp beside a blocked-off slipped damage walkway in Freeman’s Bay: we are chasing our tail on our worsening and inter-related housing, poverty and climate crises. Photo: Photo: Lynn Grieveson / The KākāTL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy ...5 days ago
A homeless person’s camp beside a blocked-off slipped damage walkway in Freeman’s Bay: we are chasing our tail on our worsening and inter-related housing, poverty and climate crises. Photo: Photo: Lynn Grieveson / The KākāTL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy ...5 days ago - Existential Crisis and Damaged Brains
 What has happened to it all?Crazy, some'd sayWhere is the life that I recognise?(Gone away)But I won't cry for yesterdayThere's an ordinary worldSomehow I have to findAnd as I try to make my wayTo the ordinary worldYesterday morning began as many others - what to write about today? I began ...5 days ago
What has happened to it all?Crazy, some'd sayWhere is the life that I recognise?(Gone away)But I won't cry for yesterdayThere's an ordinary worldSomehow I have to findAnd as I try to make my wayTo the ordinary worldYesterday morning began as many others - what to write about today? I began ...5 days ago - A speed limit is not a target, and yet…
This is a guest post from longtime supporter Mr Plod, whose previous contributions include a proposal that Hamilton become New Zealand’s capital city, and that we should switch which side of the road we drive on. A recent Newsroom article, “Back to school for the Govt’s new speed limit policy“, ...5 days ago
- The Kākā’s Pick 'n' Mix for Monday, July 22
 TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 7:00 am on Monday, July 22 are:Today’s Must Read: Father and son live in a tent, and have done for four years, in a million ...5 days ago
TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 7:00 am on Monday, July 22 are:Today’s Must Read: Father and son live in a tent, and have done for four years, in a million ...5 days ago - The Kākā’s Journal of Record for Monday, July 22
 TL;DR: As of 7:00 am on Monday, July 22, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:US President Joe Biden announced via X this morning he would not stand for a second term.Multinational professional services firm ...5 days ago
TL;DR: As of 7:00 am on Monday, July 22, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:US President Joe Biden announced via X this morning he would not stand for a second term.Multinational professional services firm ...5 days ago - 2024 SkS Weekly Climate Change & Global Warming News Roundup #29
A listing of 32 news and opinion articles we found interesting and shared on social media during the past week: Sun, July 14, 2024 thru Sat, July 20, 2024. Story of the week As reflected by preponderance of coverage, our Story of the Week is Project 2025. Until now traveling ...6 days ago
- I'd like to share what I did this weekend
 6 days ago
6 days ago - For the children – Why mere sentiment can be a misleading force in our lives, and lead to unex...
 National: The Party of ‘Law and Order’ IntroductionThis weekend, the Government formally kicked off one of their flagship policy programs: a military style boot camp that New Zealand has experimented with over the past 50 years. Cartoon credit: Guy BodyIt’s very popular with the National Party’s Law and Order image, ...6 days ago
National: The Party of ‘Law and Order’ IntroductionThis weekend, the Government formally kicked off one of their flagship policy programs: a military style boot camp that New Zealand has experimented with over the past 50 years. Cartoon credit: Guy BodyIt’s very popular with the National Party’s Law and Order image, ...6 days ago - A friend in uncertain times
 Day one of the solo leg of my long journey home begins with my favourite sound: footfalls in an empty street. 5.00 am and it’s already light and already too warm, almost.If I can make the train that leaves Budapest later this hour I could be in Belgrade by nightfall; ...6 days ago
Day one of the solo leg of my long journey home begins with my favourite sound: footfalls in an empty street. 5.00 am and it’s already light and already too warm, almost.If I can make the train that leaves Budapest later this hour I could be in Belgrade by nightfall; ...6 days ago - The Chaotic World of Male Diet Influencers
 Hi,We’ll get to the horrific world of male diet influencers (AKA Beefy Boys) shortly, but first you will be glad to know that since I sent out the Webworm explaining why the assassination attempt on Donald Trump was not a false flag operation, I’ve heard from a load of people ...6 days ago
Hi,We’ll get to the horrific world of male diet influencers (AKA Beefy Boys) shortly, but first you will be glad to know that since I sent out the Webworm explaining why the assassination attempt on Donald Trump was not a false flag operation, I’ve heard from a load of people ...6 days ago - It's Starting To Look A Lot Like… Y2K
 Do you remember Y2K, the threat that hung over humanity in the closing days of the twentieth century? Horror scenarios of planes falling from the sky, electronic payments failing and ATMs refusing to dispense cash. As for your VCR following instructions and recording your favourite show - forget about it.All ...1 week ago
Do you remember Y2K, the threat that hung over humanity in the closing days of the twentieth century? Horror scenarios of planes falling from the sky, electronic payments failing and ATMs refusing to dispense cash. As for your VCR following instructions and recording your favourite show - forget about it.All ...1 week ago - Bernard’s Saturday Soliloquy for the week to July 20
 Climate Change Minister Simon Watts being questioned by The Kākā’s Bernard Hickey.TL;DR: My top six things to note around housing, climate and poverty in Aotearoa’s political economy in the week to July 20 were:1. A strategy that fails Zero Carbon Act & Paris targetsThe National-ACT-NZ First Coalition Government finally unveiled ...1 week ago
Climate Change Minister Simon Watts being questioned by The Kākā’s Bernard Hickey.TL;DR: My top six things to note around housing, climate and poverty in Aotearoa’s political economy in the week to July 20 were:1. A strategy that fails Zero Carbon Act & Paris targetsThe National-ACT-NZ First Coalition Government finally unveiled ...1 week ago - Pharmac Director, Climate Change Commissioner, Health NZ Directors – The latest to quit this m...
 Summary:As New Zealand loses at least 12 leaders in the public service space of health, climate, and pharmaceuticals, this month alone, directly in response to the Government’s policies and budget choices, what lies ahead may be darker than it appears. Tui examines some of those departures and draws a long ...1 week ago
Summary:As New Zealand loses at least 12 leaders in the public service space of health, climate, and pharmaceuticals, this month alone, directly in response to the Government’s policies and budget choices, what lies ahead may be darker than it appears. Tui examines some of those departures and draws a long ...1 week ago - Flooding Housing Policy
 The Minister of Housing’s ambition is to reduce markedly the ratio of house prices to household incomes. If his strategy works it would transform the housing market, dramatically changing the prospects of housing as an investment.Leaving aside the Minister’s metaphor of ‘flooding the market’ I do not see how the ...1 week ago
The Minister of Housing’s ambition is to reduce markedly the ratio of house prices to household incomes. If his strategy works it would transform the housing market, dramatically changing the prospects of housing as an investment.Leaving aside the Minister’s metaphor of ‘flooding the market’ I do not see how the ...1 week ago - A Voyage Among the Vandals: Accepted (Again!)
 As previously noted, my historical fantasy piece, set in the fifth-century Mediterranean, was accepted for a Pirate Horror anthology, only for the anthology to later fall through. But in a good bit of news, it turned out that the story could indeed be re-marketed as sword and sorcery. As of ...1 week ago
As previously noted, my historical fantasy piece, set in the fifth-century Mediterranean, was accepted for a Pirate Horror anthology, only for the anthology to later fall through. But in a good bit of news, it turned out that the story could indeed be re-marketed as sword and sorcery. As of ...1 week ago - The Kākā's Chorus for Friday, July 19
 An employee of tobacco company Philip Morris International demonstrates a heated tobacco device. Photo: Getty ImagesTL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy on Friday, July 19 are:At a time when the Coalition Government is cutting spending on health, infrastructure, education, housing ...1 week ago
An employee of tobacco company Philip Morris International demonstrates a heated tobacco device. Photo: Getty ImagesTL;DR: The top six things I’ve noted around housing, climate and poverty in Aotearoa’s political economy on Friday, July 19 are:At a time when the Coalition Government is cutting spending on health, infrastructure, education, housing ...1 week ago - The Kākā’s Pick 'n' Mix for Friday, July 19
 TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 8:30 am on Friday, July 19 are:Scoop: NZ First Minister Casey Costello orders 50% cut to excise tax on heated tobacco products. The minister has ...1 week ago
TL;DR: My pick of the top six links elsewhere around housing, climate and poverty in Aotearoa’s political economy in the last day or so to 8:30 am on Friday, July 19 are:Scoop: NZ First Minister Casey Costello orders 50% cut to excise tax on heated tobacco products. The minister has ...1 week ago - Weekly Roundup 19-July-2024
Kia ora, it’s time for another Friday roundup, in which we pull together some of the links and stories that caught our eye this week. Feel free to add more in the comments! Our header image this week shows a foggy day in Auckland town, captured by Patrick Reynolds. ...1 week ago
- Weekly Climate Wrap: A market-led plan for failure
TL;DR : Here’s the top six items climate news for Aotearoa this week, as selected by Bernard Hickey and The Kākā’s climate correspondent Cathrine Dyer. A discussion recorded yesterday is in the video above and the audio of that sent onto the podcast feed.The Government released its draft Emissions Reduction ...1 week ago
- Tobacco First
 Save some money, get rich and old, bring it back to Tobacco Road.Bring that dynamite and a crane, blow it up, start all over again.Roll up. Roll up. Or tailor made, if you prefer...Whether you’re selling ciggies, digging for gold, catching dolphins in your nets, or encouraging folks to flutter ...1 week ago
Save some money, get rich and old, bring it back to Tobacco Road.Bring that dynamite and a crane, blow it up, start all over again.Roll up. Roll up. Or tailor made, if you prefer...Whether you’re selling ciggies, digging for gold, catching dolphins in your nets, or encouraging folks to flutter ...1 week ago - Trump’s Adopted Son.
 Waiting In The Wings: For truly, if Trump is America’s un-assassinated Caesar, then J.D. Vance is America’s Octavian, the Republic’s youthful undertaker – and its first Emperor.DONALD TRUMP’S SELECTION of James D. Vance as his running-mate bodes ill for the American republic. A fervent supporter of Viktor Orban, the “illiberal” prime ...1 week ago
Waiting In The Wings: For truly, if Trump is America’s un-assassinated Caesar, then J.D. Vance is America’s Octavian, the Republic’s youthful undertaker – and its first Emperor.DONALD TRUMP’S SELECTION of James D. Vance as his running-mate bodes ill for the American republic. A fervent supporter of Viktor Orban, the “illiberal” prime ...1 week ago - The Kākā’s Journal of Record for Friday, July 19
 TL;DR: As of 6:00 am on Friday, July 19, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:The PSA announced the Employment Relations Authority (ERA) had ruled in the PSA’s favour in its case against the Ministry ...1 week ago
TL;DR: As of 6:00 am on Friday, July 19, the top six announcements, speeches, reports and research around housing, climate and poverty in Aotearoa’s political economy in the last day are:The PSA announced the Employment Relations Authority (ERA) had ruled in the PSA’s favour in its case against the Ministry ...1 week ago
{kind=link}
- Speech: Chris Hipkins’ Auckland hui address
 Te Rangi e tu nei (The sky above us) Te Papa e takoto nei (The land beneath us) Tatou katoa te hunga ora (To us all the living) Tena koutou katoa (Greetings) ...2 hours ago
Te Rangi e tu nei (The sky above us) Te Papa e takoto nei (The land beneath us) Tatou katoa te hunga ora (To us all the living) Tena koutou katoa (Greetings) ...2 hours ago - Release: Charter schools to remove the rights of teachers
A late change to charter school legislation will cheat educators out of fair pay and negotiating power proving charter schools are just a vehicle to make profit out of our education system. ...24 hours ago
- Te iwi Māori will not stand for another Foreshore and Seabed
In 2004 te iwi Māori rallied against the Crown’s attempt to confiscate our coastlines and moana with the Foreshore and Seabed Act. This led to the largest hīkoi of a generation and the birth of Te Pāti Māori. 20 years later, history is repeating itself. Today the government has announced ...2 days ago
- Te Pāti Māori Acknowledge the Need for Fundamental Change in State Care
It has been five and a half years since the Royal Commission of Inquiry into Abuse in Care was established to investigate the abuse of children, young people, and vulnerable adults within state and faith-based institutions. Yesterday, the final report - Whanaketia through pain and trauma, from darkness to light ...2 days ago
- National disgrace for children in poverty
Shifting the goalposts on child poverty is a new low for the National-led government. ...2 days ago
- Release: National disgrace for children in poverty
Shifting the goalposts on child poverty is a new low for the National-led government. ...2 days ago
- Government quietly waters down child poverty targets
 The Government’s move to dilute child poverty targets is a reminder that it is actively choosing to preserve hardship for thousands of households. ...2 days ago
The Government’s move to dilute child poverty targets is a reminder that it is actively choosing to preserve hardship for thousands of households. ...2 days ago - Release: National jumps on Labour’s trains
National is so short on ideas it is now announcing Labour’s rail announcement from a year ago, Labour transport spokesperson Tangi Utikere said. ...2 days ago
- Release: Opposition parties unite to protect ECE
Labour, the Green Party and Te Pāti Māori are uniting to stop the Government’s dangerous changes to the Early Childhood Education sector. ...2 days ago
- Release: Another step forward for survivors of abuse in care
Labour welcomes the Royal Commission of Inquiry into Abuse in Care’s final report and the government committing to a formal apology in November. ...3 days ago
- Govt must listen to experiences of abuse survivors
The Government must do all it can to bring abuse in care to an end following the release of the independent inquiry. ...3 days ago
- Release: Health New Zealand exposes Minister spinning in freefall
Health New Zealand contradicted the Government’s spin that back-office bureaucracy is the cause of overspend in the public health system. ...4 days ago
- Govt must act on Israel’s illegal occupation of Palestine
The Green Party is calling on the Government to take action off the back of the International Court of Justice ruling on Israel’s illegal occupation of Palestine. ...4 days ago
- NZ Government Must Enforce ICJ Ruling
On Friday the International Court of Justice reaffirmed what Palestinian’s have been telling us for decades: that the occupation and colonisation of Palestinian lands by Israel is illegal and must end immediately. They also called for reparations for Palestinian’s who have lived under Israeli occupation since it began in 1967. ...5 days ago
- Release: Listen PM, boot camps don’t work
Refusing to listen to evidence, experts or experience the Government is stubbornly marching ahead with its boot camps. ...7 days ago
- Release: Govt must act on ICJ ruling on illegal Israeli occupation
Labour calls on the Government to act after the International Court of Justice (ICJ) ruled that Israel’s occupation of Palestinian Territories is illegal. ...7 days ago
- Release: Rents up under National, promises fall flat
National Party policies which promised to put “downward pressure” on rents are having the opposite effect. ...1 week ago
- MSD figures show Govt determined to punish beneficiaries
The 53.7 percent rise in benefit sanctions over the last year is more proof of this Government’s disdain for our communities most in need of support. ...1 week ago
- We need real solutions, not more failed boot camps – Willow-Jean Prime
Aotearoa could be a country where every child grows up feeling safe, loved and with a sense of belonging in their whānau and community. But for some of our children, this is far from reality. Instead, they are trapped in a maze of intergenerational harm that they can’t escape on ...1 week ago
- David Seymour is Unfit to Serve as Minister
Te Pāti Māori are calling for David Seymour to resign as Associate Health Minister in response to his call for Pharmac to ignore the Treaty of Waitangi. “This announcement is just another example of the government’s anti-Tiriti, anti-Māori agenda.” Said Co-leader and spokesperson for health, Debbie Ngarewa-Packer. “Seymour thinks it ...1 week ago
- Renters suffer as soaring rents feed rising inflation
The soaring price of renting is driving the rise of inflation in this country - with latest figures from Stats NZ showing rents are up 4.8 per cent on average while annual inflation is at 3.3 per cent. ...1 week ago
- National’s climate strategy undoes good progress
National’s Emissions Reduction Plan will take New Zealand further from the economy we need to ensure the next generation has a stable climate and secure livelihoods. ...1 week ago
- Green Party releases executive summary of independent investigation
Following consultation with named parties and thorough consideration of privacy interests, the Green Party is in a position to release the Executive Summary of the final report from the independent investigation into Darleen Tana. ...1 week ago
- Government back off track on climate action
Today’s Draft Emissions Reduction Plan shows the Government couldn’t care less about a liveable climate for all. ...1 week ago
- PM needs to step in over Shane Jones’ undeclared meeting
Prime Minister Christopher Luxon should be asking serious questions of his Minister for Resources Shane Jones now it’s been revealed he misled the public about a dinner with mining companies that he didn’t declare and said wasn’t pre-arranged. ...2 weeks ago
- Te Pāti Māori Opposes Three Strikes Amendment Bill
Te Pāti Māori have submitted to the Justice Select Committee against the Sentencing (Reinstating Three Strikes) Amendment Bill. The bill will further entrench racism in our justice system and fails to focus on rehabilitation. “Reinstating Three Strikes will empower a systematically racist system and exacerbate the overrepresentation of Māori in ...2 weeks ago
- Govt Determined to Make Aotearoa a Country of Disposable Renters
The Transport and Infrastructure Committee is set to make a determination on the Residential Tenancies Amendment (RTA) Bill in the coming weeks. “This legislation will give landlords the power to kick our whānau out onto the street for no reason” said Housing spokesperson, Mariameno Kapa-Kingi. “Their solution to the housing ...2 weeks ago
- Statement on retail crime Ministerial Advisory Group
“National’s campaign was about tackling crime and the best they can do is a two-year long Ministerial Advisory Group,” Labour justice spokesperson Duncan Webb said. ...2 weeks ago
- Statement from Labour education spokesperson Jan Tinetti
“There are more examples of charter schools failing their students than there are success stories. The coalition Government is driving to dismantle our public school system and instead promote a privatised, competitive structure that puts profits before kids,” Jan Tinetti said. ...2 weeks ago
- Govt Continues to Destructively Withhold Information
“This government is choosing to deliberately mislead and withhold information, keeping our people in the dark about this government’s agenda and the future of our mokopuna,” said co-leader and spokesperson for Health, Debbie Ngarewa-Packer. The call comes after the demand from the Chief Ombudsman that Associate Minister of Health, Casey ...2 weeks ago
- Statement from Labour climate change spokesperson Megan Woods
“Today’s climate announcement by Simon Watts makes clear the National Government is simply paying lip service to meeting its climate change targets,” Megan Woods said. ...2 weeks ago
- Eight ways National is making life harder for workers
National is choosing to make life harder for workers by taking away the rights our communities have fought hard for. Here's how they’re taking workers backwards. ...3 weeks ago
- Waitlists up and workforce down under National
Health New Zealand’s recent quarterly performance report shows the public health system is going backwards under the National government. ...3 weeks ago
- Joint statement from the Prime Ministers of Canada, Australia and New Zealand
 Australia, Canada and New Zealand today issued the following statement on the need for an urgent ceasefire in Gaza and the risk of expanded conflict between Hizballah and Israel. The situation in Gaza is catastrophic. The human suffering is unacceptable. It cannot continue. We remain unequivocal in our condemnation of ...18 hours ago
Australia, Canada and New Zealand today issued the following statement on the need for an urgent ceasefire in Gaza and the risk of expanded conflict between Hizballah and Israel. The situation in Gaza is catastrophic. The human suffering is unacceptable. It cannot continue. We remain unequivocal in our condemnation of ...18 hours ago - AG reminds institutions of legal obligations
Attorney-General Judith Collins today reminded all State and faith-based institutions of their legal obligation to preserve records relevant to the safety and wellbeing of those in its care. “The Abuse in Care Inquiry’s report has found cases where records of the most vulnerable people in State and faith‑based institutions were ...21 hours ago
- More young people learning about digital safety
Minister of Internal Affairs Brooke van Velden says the Government’s online safety website for children and young people has reached one million page views. “It is great to see so many young people and their families accessing the site Keep It Real Online to learn how to stay safe online, and manage ...21 hours ago
- Speech to the Conference for General Practice 2024
Tēnā tātou katoa, Ngā mihi te rangi, ngā mihi te whenua, ngā mihi ki a koutou, kia ora mai koutou. Thank you for the opportunity to be here and the invitation to speak at this 50th anniversary conference. I acknowledge all those who have gone before us and paved the ...23 hours ago
- Employers and payroll providers ready for tax changes
New Zealand’s payroll providers have successfully prepared to ensure 3.5 million individuals will, from Wednesday next week, be able to keep more of what they earn each pay, says Finance Minister Nicola Willis and Revenue Minister Simon Watts. “The Government's tax policy changes are legally effective from Wednesday. Delivering this tax ...1 day ago
- Experimental vineyard futureproofs wine industry
An experimental vineyard which will help futureproof the wine sector has been opened in Blenheim by Associate Regional Development Minister Mark Patterson. The covered vineyard, based at the New Zealand Wine Centre – Te Pokapū Wāina o Aotearoa, enables controlled environmental conditions. “The research that will be produced at the Experimental ...1 day ago
- Funding confirmed for regions affected by North Island Weather Events
The Coalition Government has confirmed the indicative regional breakdown of North Island Weather Event (NIWE) funding for state highway recovery projects funded through Budget 2024, Transport Minister Simeon Brown says. “Regions in the North Island suffered extensive and devastating damage from Cyclone Gabrielle and the 2023 Auckland Anniversary Floods, and ...1 day ago
- Indonesian Foreign Minister to visit
Indonesia’s Foreign Minister, Retno Marsudi, will visit New Zealand next week, Foreign Minister Winston Peters has announced. “Indonesia is important to New Zealand’s security and economic interests and is our closest South East Asian neighbour,” says Mr Peters, who is currently in Laos to engage with South East Asian partners. ...1 day ago
- Strengthening partnership with Ngāti Maniapoto
He aha te kai a te rangatira? He kōrero, he kōrero, he kōrero. The government has reaffirmed its commitment to supporting the aspirations of Ngāti Maniapoto, Minister for Māori Development Tama Potaka says. “My thanks to Te Nehenehenui Trust – Ngāti Maniapoto for bringing their important kōrero to a ministerial ...2 days ago
- Transport Minister thanks outgoing CAA Chair
Transport Minister Simeon Brown has thanked outgoing Chair of the Civil Aviation Authority, Janice Fredric, for her service to the board.“I have received Ms Fredric’s resignation from the role of Chair of the Civil Aviation Authority,” Mr Brown says.“On behalf of the Government, I want to thank Ms Fredric for ...2 days ago
- Test for Customary Marine Title being restored
The Government is proposing legislation to overturn a Court of Appeal decision and amend the Marine and Coastal Area Act in order to restore Parliament’s test for Customary Marine Title, Treaty Negotiations Minister Paul Goldsmith says. “Section 58 required an applicant group to prove they have exclusively used and occupied ...2 days ago
- Opposition united in bad faith over ECE sector review
Regulation Minister David Seymour says that opposition parties have united in bad faith, opposing what they claim are ‘dangerous changes’ to the Early Childhood Education sector, despite no changes even being proposed yet. “Issues with affordability and availability of early childhood education, and the complexity of its regulation, has led ...2 days ago
- Kiwis having their say on first regulatory review
After receiving more than 740 submissions in the first 20 days, Regulation Minister David Seymour is asking the Ministry for Regulation to extend engagement on the early childhood education regulation review by an extra two weeks. “The level of interest has been very high, and from the conversations I’ve been ...2 days ago
- Government upgrading Lower North Island commuter rail
The Coalition Government is investing $802.9 million into the Wairarapa and Manawatū rail lines as part of a funding agreement with the NZ Transport Agency (NZTA), KiwiRail, and the Greater Wellington and Horizons Regional Councils to deliver more reliable services for commuters in the lower North Island, Transport Minister Simeon ...2 days ago
- Government moves to ensure flood protection for Wairoa
Local Government Minister Simeon Brown has announced his intention to appoint a Crown Manager to both Hawke’s Bay Regional and Wairoa District Councils to speed up the delivery of flood protection work in Wairoa."Recent severe weather events in Wairoa this year, combined with damage from Cyclone Gabrielle in 2023 have ...3 days ago
- PM speech to Parliament – Royal Commission of Inquiry’s Report into Abuse in Care
Mr Speaker, this is a day that many New Zealanders who were abused in State care never thought would come. It’s the day that this Parliament accepts, with deep sorrow and regret, the Report of the Royal Commission of Inquiry into Abuse in Care. At the heart of this report are the ...3 days ago
- Government acknowledges torture at Lake Alice
For the first time, the Government is formally acknowledging some children and young people at Lake Alice Psychiatric Hospital experienced torture. The final report of the Royal Commission of Inquiry into Abuse in State and Faith-based Care “Whanaketia – through pain and trauma, from darkness to light,” was tabled in Parliament ...3 days ago
- Government acknowledges courageous abuse survivors
The Government has acknowledged the nearly 2,400 courageous survivors who shared their experiences during the Royal Commission of Inquiry into Historical Abuse in State and Faith-Based Care. The final report from the largest and most complex public inquiry ever held in New Zealand, the Royal Commission Inquiry “Whanaketia – through ...3 days ago
- Half a million people use tax calculator
With a week to go before hard-working New Zealanders see personal income tax relief for the first time in fourteen years, 513,000 people have used the Budget tax calculator to see how much they will benefit, says Finance Minister Nicola Willis. “Tax relief is long overdue. From next Wednesday, personal income ...3 days ago
- Paid Parental Leave improvements pass first reading
Workplace Relations and Safety Minister Brooke van Velden says a bill that has passed its first reading will improve parental leave settings and give non-biological parents more flexibility as primary carer for their child. The Regulatory Systems Amendment Bill (No3), passed its first reading this morning. “It includes a change ...3 days ago
- Rebuilding the economy through better regulation
Two Bills designed to improve regulation and make it easier to do business have passed their first reading in Parliament, says Economic Development Minister Melissa Lee. The Regulatory Systems (Economic Development) Amendment Bill and Regulatory Systems (Immigration and Workforce) Amendment Bill make key changes to legislation administered by the Ministry ...3 days ago
- ‘Open banking’ and ‘open electricity’ on the way
New legislation paves the way for greater competition in sectors such as banking and electricity, Commerce and Consumer Affairs Minister Andrew Bayly says. “Competitive markets boost productivity, create employment opportunities and lift living standards. To support competition, we need good quality regulation but, unfortunately, a recent OECD report ranked New ...3 days ago
- Charity lotteries to be permitted to operate online
Minister of Internal Affairs Brooke van Velden says lotteries for charitable purposes, such as those run by the Heart Foundation, Coastguard NZ, and local hospices, will soon be allowed to operate online permanently. “Under current laws, these fundraising lotteries are only allowed to operate online until October 2024, after which ...4 days ago
- Accelerating Northland Expressway
The Coalition Government is accelerating work on the new four-lane expressway between Auckland and Whangārei as part of its Roads of National Significance programme, with an accelerated delivery model to deliver this project faster and more efficiently, Transport Minister Simeon Brown says. “For too long, the lack of resilient transport connections ...4 days ago
- Sir Don to travel to Viet Nam as special envoy
Sir Don McKinnon will travel to Viet Nam this week as a Special Envoy of the Government, Foreign Minister Winston Peters has announced. “It is important that the Government give due recognition to the significant contributions that General Secretary Nguyen Phu Trong made to New Zealand-Viet Nam relations,” Mr ...4 days ago
- Grant Illingworth KC appointed as transitional Commissioner to Royal Commission
Minister of Internal Affairs Brooke van Velden says newly appointed Commissioner, Grant Illingworth KC, will help deliver the report for the first phase of the Royal Commission of Inquiry into COVID-19 Lessons, due on 28 November 2024. “I am pleased to announce that Mr Illingworth will commence his appointment as ...4 days ago
- NZ to advance relationships with ASEAN partners
Foreign Minister Winston Peters travels to Laos this week to participate in a series of Association of Southeast Asian Nations (ASEAN)-led Ministerial meetings in Vientiane. “ASEAN plays an important role in supporting a peaceful, stable and prosperous Indo-Pacific,” Mr Peters says. “This will be our third visit to ...4 days ago
- Backing mental health services on the West Coast
Construction of a new mental health facility at Te Nikau Grey Hospital in Greymouth is today one step closer, Mental Health Minister Matt Doocey says. “This $27 million facility shows this Government is delivering on its promise to boost mental health care and improve front line services,” Mr Doocey says. ...4 days ago
- NZ support for sustainable Pacific fisheries
New Zealand is committing nearly $50 million to a package supporting sustainable Pacific fisheries development over the next four years, Foreign Minister Winston Peters and Oceans and Fisheries Minister Shane Jones announced today. “This support consisting of a range of initiatives demonstrates New Zealand’s commitment to assisting our Pacific partners ...4 days ago
- Students’ needs at centre of new charter school adjustments
Associate Education Minister David Seymour says proposed changes to the Education and Training Amendment Bill will ensure charter schools have more flexibility to negotiate employment agreements and are equipped with the right teaching resources. “Cabinet has agreed to progress an amendment which means unions will not be able to initiate ...4 days ago
- Commissioner replaces Health NZ Board
In response to serious concerns around oversight, overspend and a significant deterioration in financial outlook, the Board of Health New Zealand will be replaced with a Commissioner, Health Minister Dr Shane Reti announced today. “The previous government’s botched health reforms have created significant financial challenges at Health NZ that, without ...5 days ago
- Minister to speak at Australian Space Forum
Minister for Space and Science, Innovation and Technology Judith Collins will travel to Adelaide tomorrow for space and science engagements, including speaking at the Australian Space Forum. While there she will also have meetings and visits with a focus on space, biotechnology and innovation. “New Zealand has a thriving space ...5 days ago
- Climate Change Minister to attend climate action meeting in China
Climate Change Minister Simon Watts will travel to China on Saturday to attend the Ministerial on Climate Action meeting held in Wuhan. “Attending the Ministerial on Climate Action is an opportunity to advocate for New Zealand climate priorities and engage with our key partners on climate action,” Mr Watts says. ...5 days ago
- Oceans and Fisheries Minister to Solomons
Oceans and Fisheries Minister Shane Jones is travelling to the Solomon Islands tomorrow for meetings with his counterparts from around the Pacific supporting collective management of the region’s fisheries. The 23rd Pacific Islands Forum Fisheries Committee and the 5th Regional Fisheries Ministers’ Meeting in Honiara from 23 to 26 July ...7 days ago
- Government launches Military Style Academy Pilot
The Government today launched the Military Style Academy Pilot at Te Au rere a te Tonga Youth Justice residence in Palmerston North, an important part of the Government’s plan to crackdown on youth crime and getting youth offenders back on track, Minister for Children, Karen Chhour said today. “On the ...7 days ago
- Nine priority bridge replacements to get underway
The Government has welcomed news the NZ Transport Agency (NZTA) has begun work to replace nine priority bridges across the country to ensure our state highway network remains resilient, reliable, and efficient for road users, Transport Minister Simeon Brown says.“Increasing productivity and economic growth is a key priority for the ...1 week ago
- Update on global IT outage
Acting Prime Minister David Seymour has been in contact throughout the evening with senior officials who have coordinated a whole of government response to the global IT outage and can provide an update. The Department of the Prime Minister and Cabinet has designated the National Emergency Management Agency as the ...1 week ago
- New Zealand, Japan renew Pacific partnership
New Zealand and Japan will continue to step up their shared engagement with the Pacific, Foreign Minister Winston Peters says. “New Zealand and Japan have a strong, shared interest in a free, open and stable Pacific Islands region,” Mr Peters says. “We are pleased to be finding more ways ...1 week ago
- New infrastructure energises BOP forestry towns
New developments in the heart of North Island forestry country will reinvigorate their communities and boost economic development, Regional Development Minister Shane Jones says. Mr Jones visited Kaingaroa and Kawerau in Bay of Plenty today to open a landmark community centre in the former and a new connecting road in ...1 week ago
- 'Pacific Futures'
President Adeang, fellow Ministers, honourable Diet Member Horii, Ambassadors, distinguished guests. Minasama, konnichiwa, and good afternoon, everyone. Distinguished guests, it’s a pleasure to be here with you today to talk about New Zealand’s foreign policy reset, the reasons for it, the values that underpin it, and how it ...1 week ago
- 'Enough is enough' – Chris Hipkins blasts government over Māori policies
 Labour Party leader Chris Hipkins says the coalition government is unfairly targeting Māori: "Each week they find new ways to keep Māori down." ...2 hours ago
Labour Party leader Chris Hipkins says the coalition government is unfairly targeting Māori: "Each week they find new ways to keep Māori down." ...2 hours ago - Focus on Politics: Abuse in care report delivers demands for justice
The government has promised to listen to survivors, but how it responds and whether justice is served remains to be seen. ...7 hours ago
- Green AGM: Party processes will be respected on Darleen Tana issue, Chlöe Swarbrick says
A Green Party member is concerned that proper process will not be followed - but the party's co-leader says a vote will not be forced. ...7 hours ago
- Short story: Fire Engines, by Gina Butson
 Last summer when Matairangi burned, Ginny and Tom stood at the window of their lounge, watching kākā shoot skyward from the burning trees. From the distance, they looked to Ginny like pages torn from books and thrown into a bonfire. It was Tom, voice tight, who told her it was ...7 hours ago
Last summer when Matairangi burned, Ginny and Tom stood at the window of their lounge, watching kākā shoot skyward from the burning trees. From the distance, they looked to Ginny like pages torn from books and thrown into a bonfire. It was Tom, voice tight, who told her it was ...7 hours ago - Alice Munro’s shocking silence
Opinion: The Canadian short story writer Alice Munro – winner of the Nobel Prize in Literature in 2013 – died in May at the age of 92. Her work was about “the damage people inflict on one another in the name of love”, Deborah Treisman wrote in the New Yorker. ...7 hours ago
- Re-writing the timeline of the universe
This month marks two years since the most powerful telescope ever built sent its first pictures back to earth. From its lofty vantage point, beyond the moon in orbit around the sun, the James Webb Space Telescope was tuned to observe the first stars and galaxies being born soon after ...7 hours ago
- Anne Salmond: What track was that?
Comment: After Climate Change Minister Simon Watts’ preview several weeks ago, I had some optimism about the Government’s emissions reduction plan. Now I’ve read the discussion document, that hope has been dashed. How can the Government propose a plan that wants to take New Zealand taxpayers’ hard-earned money, and spend ...7 hours ago
- The Secret Diary of .. NZ’s Olympics hopefuls
Christopher Luxon: hurdles The little man from National jumps hurdles in his sleep. He’s quite good at it in his dreams and even though the reality doesn’t quite match up you have to give him credit for getting up every morning and crashing into the very first hurdle of the ...7 hours ago
- Finally heard, seen – and believed
Comment: It was a good two hours into the conversation when Tyrone Marks raised the most basic of questions when I first spoke to him in 2017. “They didn’t explain the things they did to me. They never told me why. And they still haven’t. There’s no explanation for it. ...7 hours ago
- The Weekend: If in doubt, go to the funeral
 Madeleine Chapman rounds out Death Week on The Spinoff with a final recommendation. You can read all of our Death Week coverage here. Nothing forces you to reflect on your life and relationships quite like proximity to death. For those whose nearest and dearest have died, there are reasonably obvious ...8 hours ago
Madeleine Chapman rounds out Death Week on The Spinoff with a final recommendation. You can read all of our Death Week coverage here. Nothing forces you to reflect on your life and relationships quite like proximity to death. For those whose nearest and dearest have died, there are reasonably obvious ...8 hours ago - ‘What a privilege’: Whitney from The Traitors NZ on life as a funeral director
Whitney Greene takes us through her life in television, including the TV character she’d like to plan a funeral for and her cow lung catastrophe on The Traitors NZ. “If the phone rings, I have to answer it,” Whitney Greene from The Traitors NZ warns as we begin our My ...8 hours ago
- Rich and rare: Bad Archive by Flora Feltham, reviewed
Maddie Ballard reviews the debut essay collection of Pōneke writer Flora Feltham. In ‘The Raw Material’, the longest essay in Flora Feltham’s dazzling debut collection, the author heads out for a run after hours of weaving and sees the world turn to textile. “Pounding along the Parade, I saw the ...8 hours ago
- ‘Possibly the best live gig I have been to’: TRiPS’ perfect weekend playlist
Andy Christiansen, one half of the experimental rock-pop duo TRiPS, shares the tunes inspiring the band’s perfect weekend and new release. “Good speakers, good food, good music, no distractions”: that’s all you need to enjoy the psychedelic stylings of TRiPS, a new band formed by Fly My Pretties’ Barnaby Weir ...8 hours ago
- Every sport at the Paris Olympics, ranked from least to most fun to watch
Celebrating our quadrennial opportunity to become experts in a bunch of sports we never normally watch. The games of the XXXIII Olympiad are upon us. Paris will host this year’s showcase of sporting and athletic prowess, which means some late-night and early-morning viewing for us in Aotearoa. But what sports ...8 hours ago
- The Sunday Essay: Remembering my brother
The photograph is striking and beautiful, but also disturbing – a reminder that my love for John was often entangled in shame. The Sunday Essay is made possible thanks to the support of Creative New Zealand. In the spring of 1980, in Dunedin, shortly before his death, someone took a photograph ...8 hours ago
- Dog of the month: Babushka, who is notorious in Newtown
Get to know Babushka, our latest Dog of the Month. This feature was offered as a reward during our What’s Eating Aotearoa PledgeMe campaign. Thank you to Babu’s humans, Jo and Isabel, for their support. Dog name: Babushka (Babu for short) Age: 2 Breed: Border Collie X poodle If rescued, ...8 hours ago
- Photojournalist targeted by Israeli army carries Olympic torch in Paris
 Pacific Media Watch A Lebanese photojournalist who was severely wounded during an Israeli air strike in south Lebanon carried the Olympic torch in Paris this week in honour of her peers who have been wounded and killed in the field — especially in Gaza and Lebanon. Christina Assi of Agence ...15 hours ago
Pacific Media Watch A Lebanese photojournalist who was severely wounded during an Israeli air strike in south Lebanon carried the Olympic torch in Paris this week in honour of her peers who have been wounded and killed in the field — especially in Gaza and Lebanon. Christina Assi of Agence ...15 hours ago - 70 years on from tests, Marshallese women still fight for nuclear justice
The first report in a five-part web series focused on the 15th Triennial Conference of Pacific Women taking place in the Marshall Islands this week. SPECIAL REPORT: By Netani Rika in Majuro Women continue to fight for justice 70 years after the first nuclear tests by the United States caused ...16 hours ago
- 'Israel must listen' – Luxon, Albanese, Trudeau issue joint support for US-backed ce...
Christopher Luxon has joined with Australia and Canada's leaders in voicing support for US President Joe Biden's ceasefire deal between Israel and Hamas. ...17 hours ago
- Politics with Michelle Grattan: ‘Teal’ Zoe Daniel on political donations, representing Jewish vo...
Source: The Conversation (Au and NZ) – By Michelle Grattan, Professorial Fellow, University of Canberra The 2022 election brought the “teal wave” into parliament. The next election will test whether teals, who occupy what were Liberal seats, and other independents can maintain their momentum. Joining us on the Podcast ...17 hours ago
- China: still the world’s biggest emitter, but also an emerging force in climate diplomacy
Source: The Conversation (Au and NZ) – By Xu Yi-chong, Professor of Governance and Public Policy, Griffith University fuyu liu, Shutterstock Seven years seems a lifetime in politics. In 2017, President Donald Trump announced the United States would withdraw from the Paris Agreement. It prompted Canada, China and the ...17 hours ago
- Federal Court finds insufficient evidence Roundup weedkiller causes cancer. What does the science sa...
Source: The Conversation (Au and NZ) – By Ian Musgrave, Senior lecturer in Pharmacology, University of Adelaide Pixavri/Shutterstock A major Federal Court class action has been dismissed this week after Justice Michael Lee ruled there was not enough evidence to prove the weedkiller Roundup causes cancer. Plaintiff Kelvin ...18 hours ago
- The Week in Politics: Parliament set a vital task, Darleen Tana returns
In The Week in Politics: politicians have to decide what to do about child abuse, Health NZ is booked in for major surgery and Darleen Tana returns. ...18 hours ago
- Māori leader says government's controversial boot camps the wrong approach
Meihana Durie is concerned a camp draws from methodology popularised by the US marines. ...19 hours ago
- Twice as good for half the respect: Kamala Harris’ battle for the White House
Source: The Conversation (Au and NZ) – By Clare Corbould, Associate Professor, Contemporary Histories Research Group, Deakin University Mainstream media are surprisingly muted at the prospect of the world’s most powerful nation being led for the first time by a woman – specifically a woman of colour, Vice President Kamala ...19 hours ago
- Drone food delivery is spreading across Australia. Research suggests we will eat more junk food as a...
Source: The Conversation (Au and NZ) – By Rebecca Bennett, PhD Student, Associate Research Fellow, Deakin University Last week, a drone delivery company called Wing (owned by Google’s parent company, Alphabet) started operating in Melbourne. Some 250,000 residents in parts of the city’s eastern suburbs can now order food from ...19 hours ago
- Our research shows 4 in 10 Australians in aged care are malnourished. What can we do about it?
Source: The Conversation (Au and NZ) – By Jonathan Foo, Lecturer, Physiotherapy, Monash University pikselstock/Shutterstock In the next 40 years in Australia, it’s predicted the number of Australians aged 65 and over will more than double, while the number of people aged 85 and over will more than triple. ...19 hours ago
- Before there was diving and relays, there was the Poetry Olympics
Source: The Conversation (Au and NZ) – By Katrina Grant, Research Associate, Power Institute for Arts and Visual Culture, University of Sydney Jonas Åkerström’s 1790 work, Session of the Accademia dell’Arcadia on August 17 1788. Nationalmuseum/Cecilia Heisser Ever wondered whether you’d have a better chance at winning an Olympic gold ...20 hours ago
- Abuse in Care inquiry: Judith Collins warns of possible prosecutions if records destroyed
Judith Collins is reminding all state and faith-based institutions of their legal obligation to preserve records. ...20 hours ago
- Health star labels move closer to being mandatory. But food companies could still (legally) game the...
Source: The Conversation (Au and NZ) – By Alexandra Jones, Program Lead, Food Governance, George Institute for Global Health wavebreakmedia/Shutterstock On Thursday, Australian and New Zealand food ministers at state, federal and national levels met to thrash out what’s next for health star ratings on packaged foods. Now, after ...21 hours ago
- Abuse in Care inquiry: Call for Pacific focused redress pathway
The Abuse in Care report found many Pacific survivors lost their connections to their culture and language, resulting in trauma that has been carried from generation to generation. ...21 hours ago
- Education Review Office Pragmatism Will Really Help The Sector While The Regulation Review Is Underw...
 In the regulatory review, ECC intends to suggest that ERO focus on curriculum delivery reviews rather than the Ministry, because it’s not efficient or effective to have two agencies with radically different approaches climbing over each other. ...22 hours ago
In the regulatory review, ECC intends to suggest that ERO focus on curriculum delivery reviews rather than the Ministry, because it’s not efficient or effective to have two agencies with radically different approaches climbing over each other. ...22 hours ago - Watch: Christopher Luxon's security cut short visit ahead of protest
The prime minister was speaking to reporters during a walkabout with police in central Auckland. ...23 hours ago
- Christopher Luxon calls for witnesses to alleged '80s politician paedophile ring to speak out
Christopher Luxon says anyone with evidence about claims involving politicians and civil servants in the 1980s should go to police. ...23 hours ago
- Co-chairs Of Te Rūnanga Nui O Ngā Kura Kaupapa Māori Welcome The Waitangi Tribunal Report –...
Te Rūnanga Nui o Ngā Kura Kaupapa Māori invites the current government to work in partnership with them to develop a pathway forward, including the development of a parallel pathway and meaningful policy and strategy for Kura Kaupapa Māori ...23 hours ago
- Why this season of The Traitors is the best reality TV NZ has ever made
If you haven’t started watching yet, Tara Ward begs you to reconsider. This is an excerpt from our weekly pop culture newsletter Rec Room. Sign up here. In the world of New Zealand reality television, we have many gems in our crown. There’s the delicious second season of the Celebrity Treasure ...23 hours ago
- The Friday Poem: ‘The clothes of the dead’ by Fiona Kidman
A new poem by Fiona Kidman. The clothes of the dead I did not keep my mother’s furry red beret for long nor the stringy scarves that adorned the necks of my aunts, although I have kept tag ends of gold, the rings and trinkets they wore, the brooches no ...23 hours ago
- Ngāi Tahu Challenges Changes To MACA
The government’s announcement that it will re-open the foreshore and seabed controversy by changing the rules on recognising centuries-old Māori customary title for a third time goes against the rule of law and New Zealand values,” Mr Tipa says. ...23 hours ago
- The Unity Books bestseller chart for the week ending July 26
The only published and available best-selling indie book chart in New Zealand is the top 10 sales list recorded every week at Unity Books’ stores in High St, Auckland, and Willis St, Wellington. AUCKLAND 1 Lioness by Emily Perkins (Bloomsbury, $25) Roarrrr! Perkins’ brilliant, award-winning, Marian-Keyes anointed, darkly funny, long ...23 hours ago
- Overturning Court Of Appeal Decision On Foreshore And Seabed Is Abuse Of Power
The 2004 Act vested ownership of the foreshore and seabed in the Crown, extinguishing any Māori claims to ownership and causing widespread outrage and protests among Māori communities. ...23 hours ago
- Gang crackdown: why anti-patch policies backfire – and what would actually work
Source: The Conversation (Au and NZ) – By Antje Deckert, Associate Professor (Criminology), Auckland University of Technology Getty Images Despite the connection between institutional harm and gang membership made clear in this week’s mammoth royal commission abuse-in care report, the government seems unlikely to soften its “get tough on ...23 hours ago
- Watch: Christopher Luxon's security cut short visit short ahead of protest
The prime minister was speaking to reporters during a walkabout with police in central Auckland. ...24 hours ago
- Overruling court on coastal rights risks new protests, Te Pāti Māori warns
Te Pāti Māori is warning a move to overturn a court decision risks a return of the big foreshore and seabed protests of 20 years ago. ...24 hours ago
- New Zealanders in action: When and who to watch in week one of the Paris Olympics
From Lewis Clareburt in the swimming to the start of the rowing – the first seven days of Paris 2024 promise to be big for New Zealand. There are few events that bring the country together quite like an Olympic Games. Nothing quite matches the excitement of getting up in ...1 day ago
- The local science that just made a huge cameo in The Kardashians
Groundbreaking local science just showed up in the most surprising of places: the season finale of The Kardashians. In the season five finale of The Kardashians last night, several members of the family gathered together in one of their signature empty, cream-coloured rooms to hear test results that had been ...1 day ago
- Can Israel and Hezbollah be pulled back from the brink of war?
Source: The Conversation (Au and NZ) – By Amin Saikal, Emeritus professor of Middle Eastern and Central Asian Studies, Australian National University The Middle East is on the brink of a possibly devastating regional war, with hostilities between Israel and Hezbollah reaching an extremely dangerous level. Washington has engaged in ...1 day ago
- Lupus is more common and severe in Aboriginal and Torres Strait Islander peoples. Learning why is cr...
Source: The Conversation (Au and NZ) – By Laura Elizabeth Eades, Rheumatologist, Monash University Lupus is an inflammatory autoimmune illness, where the body’s immune system mistakenly attacks itself. Lupus can affect virtually any part of the body, although it most commonly affects the skin, joints and kidneys. The symptoms ...1 day ago
- Government Fails To Recognise Parallels Between Whakapakari And Its Boot Camps
A law firm that specialises in working with survivors of abuse in State care is disappointed that the Government fails to recognise that its boot camps can be directly compared to previous boot camps from the 1990s and 2000s. ...1 day ago
- Crown breached Treaty principles in school reform – Waitangi Tribunal
A Waitangi Tribunal report has found the Crown breached Treaty principles in its review and reform of schools between 2018 and 2022. ...1 day ago
- Zero stars: Rating the experience of death and dying in Aotearoa
Dying is a natural part of life, like updating your Wof or seeing your hairdresser, but without the word-of-mouth recs that help guarantee a good service. What if we changed that? Dying Reviews received by The Spinoff have had the names of organisations redacted while Hospice NZ collects further data. ...1 day ago
- Not one, but two meteor showers are about to peak – here’s how to catch the stellar show
Source: The Conversation (Au and NZ) – By Jonti Horner, Professor (Astrophysics), University of Southern Queensland Mike Lewinski/Flickr, CC BY On any clear night, if you gaze skywards long enough, chances are you’ll see a meteor streaking through the sky. Some nights, however, are better than others. At ...1 day ago
- Ministry of Education puts 100 school building projects on ice
Deferring the builds and rescoping 110 others will save $2 billion, the ministry says. ...1 day ago
- How Tāmaki Makaurau became home to the world’s only lesbian museum
Despite having no bars or other designated spaces for lesbians, Auckland boasts a small but mighty lesbian museum. So how did it get here? The past 18 months has brought increasing hostility towards the queer community across Aotearoa. Kellie-Jay Keen-Minshull’s anti-trans rally in Tamaki Makaurau last March led to a ...1 day ago
- Protest At French Embassy Calls Out Hypocrisy In Kanaky As Paris Olympics Begin
Poneke Antifascist Coalition has invited Wellingtonians to stand in solidarity with the Kanak people at 12pm today outside the French Embassy in Wellington. ...1 day ago
- Chicken wire, AI and mobile phones on sticks: how the drone war in Ukraine is driving a fierce battl...
Source: The Conversation (Au and NZ) – By Peter Layton, Visiting Fellow, Strategic Studies, Griffith University Drones are the signature technology of the Ukraine war. A few miniature aircraft designs were used in the war’s early days, but an incredible array of drones have now evolved. There are different types, ...1 day ago
- What happens in my brain when I get a migraine? And what medications can I use to treat it?
Source: The Conversation (Au and NZ) – By Mark Slee, Associate Professor, Clinical Academic Neurologist, Flinders University Francisco Gonzelez/Unsplash Migraine is many things, but one thing it’s not is “just a headache”. “Migraine” comes from the Greek word “hemicrania”, referring to the common experience of migraine being predominantly ...1 day ago
- How old, inefficient housing and time-of-use electricity rates are leaving some households worse off
Source: The Conversation (Au and NZ) – By Lee White, Senior Lecturer and Horizon Fellow, School of Social and Political Sciences, University of Sydney Australia was slow to introduce minimum building standards for energy efficiency. The Nationwide House Energy Rating Scheme (NatHERS) only came into force in 2003. Older homes ...1 day ago
- Landmark new research shows how global warming is messing with our rainfall
Source: The Conversation (Au and NZ) – By Steven Sherwood, Professor of Atmospheric Sciences, Climate Change Research Centre, UNSW Sydney The past century of human-induced warming has increased rainfall variability over 75% of the Earth’s land area – particularly over Australia, Europe and eastern North America, new research shows. ...1 day ago
- Timber venues, river swimming and re-use: how the Paris Olympics is going green – and what it’s ...
Source: The Conversation (Au and NZ) – By Tony Heynen, Program Coordinator, Sustainable Energy, The University of Queensland A temporary stadium in the Champ-de-Mars, Paris Ekaterina Pokrovsky/Shutterstock As Paris prepares to host the Olympic and Paralympic Games, the sustainability of the event is coming under scrutiny. The organisers have promoted ...1 day ago
- An Ode to Newtown Sports Bar, Wellington’s last great pub
A night of karaoke and community in a pub that feels like a memory. You’d barely even notice it, unless you knew to look. Tucked away behind a liquor store on busy Constable Street is the capital’s last great pub. Newtown Sports Bar is an emblem of the pub culture ...1 day ago
- Health commissioner in meetings over new Dunedin Hospital cost blowout
The spotlight will then turn on the proposed new regional hospitals for Nelson, Hawke’s Bay, Tauranga and Palmerston North The post Health commissioner in meetings over new Dunedin Hospital cost blowout appeared first on Newsroom. ...1 day ago
- Declining PhD student numbers are a warning sign for NZ’s future knowledge economy
Source: The Conversation (Au and NZ) – By Ian Wright, Professor in Marine Geology, University of Canterbury Louise Corcoran/Getty Images The decline in the number of doctoral candidates at New Zealand universities is a worrying sign for the country’s effort to build a knowledge-based economy. Aotearoa New Zealand’s ...1 day ago
- Migrant workers have long been too scared to report employer misconduct. A new visa could change thi...
Source: The Conversation (Au and NZ) – By Laurie Berg, Associate Professor, University of Technology Sydney defotoberg/Shutterstock Migrant worker exploitation is entrenched in workplaces across Australia. Tragically, a deep fear of immigration consequences means most unlawful employer conduct goes unreported. On Wednesday, however, the government officially launched a ...1 day ago
- The chaotic history of the Olympics in Paris, where one games nearly ended the movement – and the ...
Source: The Conversation (Au and NZ) – By Vaughan Cruickshank, Senior Lecturer in Health and Physical Education, University of Tasmania Paris is about to host its third summer Olympics. While we don’t yet know what the legacy of this year’s games will be, let’s take the opportunity to reflect on ...1 day ago
- ‘Bloodbath’, ‘bullseye’, ‘America’s Hitler’: why has our political rhetoric gotten so ...
Source: The Conversation (Au and NZ) – By Hugh Breakey, Deputy Director, Institute for Ethics, Governance & Law, Griffith University In the wake of the assassination attempt on former US President Donald Trump, there were calls from both sides of US politics, as well as internationally, to reduce the brutal, ...1 day ago
- Politics, security and the Seine: where the Paris Olympics’ flashpoints will be
Source: The Conversation (Au and NZ) – By Keith Rathbone, Senior Lecturer, Modern European History and Sports History, Macquarie University Two high-profile assaults on Australians in Paris have raised concerns about security ahead of the Olympic Games. On Saturday evening, a young woman was allegedly sexually assaulted by a ...1 day ago
- Leaked Health NZ restructure proposal shines light on latest job cuts
There's "shock and dismay" at the health body with another "brutally fast" round of redundancies looming, one insider says. ...1 day ago
- Revisiting the cost of dying
Dying is inevitable and, so it seems, is it costing a lot, writes Stewart Sowman-Lund in today’s extract from The Bulletin. To receive The Bulletin in full each weekday, sign up here. The cost of dying ...1 day ago
- The state care decision that rippled through four generations
The government took Joyce Harris's first baby and sent her off to a girls' home. Half a century on - and out of oceans of hurt - it asked her to be a mother figure. ...1 day ago
- Mt Victoria Tunnel, Basin Reserve plans: NZTA spent seven times more on consultants than on its own ...
Staff working on a second Mt Victoria Tunnel and the Basin Reserve upgrade were paid $175,000 - but consultants were paid nearly $1.3 million. ...1 day ago
- Will Gen X ever be able to retire?
Caught between ageing parents and struggling kids, retirement planning is tough for a whole generation. ...1 day ago
- Minister defends lowered child poverty targets as 'achievable'
Louise Upston has rejected criticisms of lowered child poverty reduction targets, saying they are achievable and ambitious. ...1 day ago
- What is the wildest Brokenwood Mysteries death of all time?
It’s the deadliest fictional town in the country, but which death has been the most bonkers? Alex Casey looks back at 10 seasons of The Brokenwood Mysteries to find out. Warning: The following ranking story contains famous New Zealand actors appearing to be dead (not alive). The Spinoff has been ...1 day ago
- ‘It’s a no-brainer’: Why Aotearoa needs to ride the wave of water cremation
Water cremation is the biggest thing to happen to the death industry in the last 100 years. Alex Casey meets the people trying to bring it to Aotearoa. Through a set of mirrored doors down the industrial end of Christchurch’s St Asaph Street, death is getting a new lease on ...1 day ago
- All-powerful Levy is feudal baron of a $28b fiefdom
Opinion: New Health NZ commissioner Lester Levy is authorised to assume operational leadership – chief executive Margie Apa is effectively relegated to his operational deputy The post All-powerful Levy is feudal baron of a $28b fiefdom appeared first on Newsroom. ...1 day ago
Crazy to my mind, yes. Arguing the toss, yes. Perhaps dated (giving them the benefit of the doubt)
Letter was written in early November, accepted by NZMC in early Dec and published 22/12.
They will be heaping mana on themselves by getting a letter published in NZMC. Other seemingly august publications will pick this up as if it has some imprimatur from NZMC.
I have deleted the names of the authors, they are at the top of the article and I do not want to to give them any credence. Plan B is the best name.
This from MS summarises it well.
First impression is they are a group of 'self-regarding academics' who want to be noticed and have some attention going their way. They seem to not be happy the experts we have come to listen to and respect are getting too much media attention and think they know better. Well done Michael Baker for his robust response.
Could also be driven from economic beliefs.
Could also be driven by the economic beliefs of whoever is funding them.
It is common and good (!) practice for authors of a peer-reviewed Research Article to acknowledge all the funding sources that enabled the present work and publication.
At the end of their letter they claim to have received no specific funding for producing their letter.
Of course, that doesn't preclude influence from the funding sources for their other work. Or maybe they really are spreading their nuttery around for free
from the goodness of their heartsfor undetermined reasons.From the Journal website:
https://www.publish.csiro.au/hc/forauthors/AuthorInstructions#22
https://www.publish.csiro.au/hc/forauthors/AuthorInstructions#23
Looks like Thornley ended a job advising an international airport on covid risks, then. He declared it for a September publication:
Or he now doesn't think it's a "competing interest".
That was then, now is now 😉
Just as a response I should declare the following on behalf of the Standard.
Sponsorships
None except for the occasional donation and LPrent hosting the server and paying for the broadband.
Payments associated with the writing of this post
I wish …
Competing interests
Only that I want to see a safe and secure Aotearoa.
lol
There is a National party influence at Auckland University – one of their senior academics Des Gorman was a sidekick of a former Treasury boss Murray Horn on National appointed positions in National Health oversight – National Health Board. These two were arguing for taking management of the pandemic off MOH earlier this year (and against lockdowns as well).
Horn was at Treasury during the sweeping economic reforms of the fourth Labour government in the 1980s, and served as Treasury secretary during the welfare and labour reforms of the 1990s National government. His book in 1998 championed making neo-liberal reforms that future governments would be unable to undo.
Apophenia (HT to McFlock).
Hardly, former National appointees were peddling National Party/business lines. And also offering to take over pandemic management – inferring lack of confidence in the government and MOH.
An obvious fear being a successful lockdown elimination strategy would end National's election hopes.
😀
Has it occurred to you that National Party/business might have been peddling lines of former National appointees?
Anyway, you replied saying “[t]here is a National party influence at Auckland University” to a (rhetorical?) question about the “economic beliefs of whoever is funding them [Plan B activists]”. So, where and what is that influence, specifically?
This mythical ‘influence’ doesn’t seem to affect the likes of Siouxsie Wiles, Shaun Hendy, Dame Anne Salmond, Margaret Mutu, to name a few. Are you guilty of apophenia to suit your (inner?) narrative, by any chance?
Professor Baker’s words are still fresh in my mind …
Yup, it was their only hope and they were such a shambolic lot that I doubt that anything would have saved them. Imagine a failed lockdown elimination strategy and National now leading Government! The mind boggles!
Well yuh and he is Des Gorman – a very senior figure there – above Thornley, "Sundecorp" and co and an appointee alongside Horn on the National Health Board for years during the 2009-2017 period.
As I said Gorman and Horn opposed lockdowns and wanted an appointed body to take over the response from MOH (people like themselves). Which is in line with the ideological direction of the right internationally – team Barrington and the Telegraph freedom line. No lockdown and undermining state led response, our Team B as it were.
It’s example, and precedent led influence.
National are well known for appointing their ideologues into sinecure, such as NHB. And corporates are well known for funding research by those they think are of similar ideology – for example those who fund the New Zealand Initiative.
Those who are unable to note connections between events, never understand anything about anything. Nor learn from history.
And those who bare grudges from the past and carry them from one issue onto another, rather than take on the matter at hand directly, rarely realise anything constructive – they just see targets.
Note, or imagine?
Churchill imagined the German military build up in the 1930's was a real threat for years …
WHO issued a world alert of a pandemic back in 2016 …
Churchill was receiving confidential intelligence material through connections he'd made in his previous government roles. He was talking about a build up because he'd seen the evidence of actual soldiers, ships, tanks, and aircraft. The connections were part of the picture: new ships are evidence of new shipbuilding. New machine guns are evidence of rearming. More divisions are evidence of bigger armies.
WHO has given pandemic warnings based on experimental, epidemiological, and historical evidence weighted towards the hazards of novel viruses entering a population based around frequent global migration. The connections were part of the picture. Mutation rates and migration rates and delays in novel virus identification all point towards significant spread before measures can be implemented.
You've provided a lot of dots selectively, there are many missing dots (all the leftish academics), and zero actual connections between these guys and specific payment for their work.
No its less the evidence than the breadth of perspective in play.
Other right wingers had the same information as Churchill – but they liked the way Hitler put down the left in Germany and saw him as weapon against Russia. They were blinded by ideology.
Their's was a short term or current events led position, Churchill was more focused on the history of it all. And the fact that WW1 was supposedly the war that ushered in democracy.
The point being that Churchill was noting connections and basing his projections on clear indications, rather than taking a bunch of random events and constructing his own narrative around them – to the point of ignoring evidence that could equally support the opposite perspective.
So he saw new battleships and built a picture of rearming, just as he might see the number of nats in a university faculty and see nat bias. But there were no indications that the Nazis were disarming, while university faculties also have many leftish members.
Back then some on the left cared more about peace than democracy or collective security. And some on the right pretended to care for peace too, but were just using that to give Hitler his head.
And yes there are left and right wingers at the university today. And they have the same facts, yet the right wingers choose to oppose lockdowns – Gorman was the senior figure at Auckland and a National Party appointee on the National Health Board (and what was Horn's expertise in Health … his right wing ideology …).
When ideology is rewarded …
You know, when you have to invoke Churchill, Hitler, and WHO to demonstrate your point about National Party influence in the University of Auckland on Plan B academics specifically, it is obvious that your argument is weak as piss or non-existent altogether.
Gorman, Thornley, Sund et al (those in their economics department as well). The right wing ideology force is strong there.
Of course the peddling of right wing ideology and getting appointed to say the National Health Board (such as Horn) by National/ACT is an influence across all academia. Not just Auckland, but it is well Auckland.
Just because other people have also flirted with Team B, apparently convinced by the strength of their argumenret, if not their ideology, does not refute that.
While I supported the lockdown to get spread under control to protect the health system, and get testing and tracing up to scratch. For a week or two I had doubts about going for elimination, then I thought it through and saw the light. Puting the people first, before the economy was not only right – but it would work and possibly lead to political change. Little wonder the right were nervous.
There’s rightwing ideology in the Economics Dept? Well, strike me down with a feather!
Isn’t Tim Hazledine a Professor in that Department too? And Professor Jilnaught Wong (different Dept, same Faculty) who called upon NZ businesses to pay back the Wage Subsidy?
Maybe the World is a little more complex and nuanced than your narrative, yes?
So thousands of years ago people imagined pictures within an essentially random pattern of dots in the night sky. They noticed a connection between those constellations and seasons. All good. Then they imagined stories based on those pictures and connections, and astrology was born.
All you're doing is listing bright points in the night sky, and ignoring others that don't fit your story. But the stories are getting more elaborate the more this is pointed out.
Saying that right wing ideology is rewarded by both business (who funds New Zealand Initiative) and National (political appointments), is hardly a unique argument, nor often so disputed. And it seems that puting the economy first line, or freedom first (political line alongside the economic one) has an impact even on health academics – if they do not place the public good first.
Apophenia, astrology – you two are hilarious, the Soviet gulag meets must not be quarrelsome against the CCP. Not playing some KB pantomine stereotype of TS?
In general, yes. Just as the left wing have been known to fund research and support people with left wing ideaology (e.g. unions, some left wing political parties).
But you made a connection between a specific body of research a specific organisation. That requires a specific identified connection.
Lots of people suspected some nats and right wing bloggers were in cahoots, but that wasn't a demonstrable fact until a specific connection in the form of hacked emails was made public.
Thornley has already declared himself to have had paid work (at some time during this pandemic) advising a business that specialised in international travel. Dunno why you need to drag the nats into it – I doubt this lot would have been able to keep a nod and a wink secret, anyway.
Very well said, thank you.
QFT
Somehow, I don’t think that SPC will come to the party though 🙁
You have not presented anything that points to a direct influence, undue or otherwise, of the National Party within the University of Auckland on Plan B academics. Incidentally, not all Plan B academics are from the University of Auckland so that mythical ‘influence’ must reach far & wide, maybe it’s a conspiracy?
Des Gorman works in a different School and Department from Simon Thornley so he has no seniority as such over Thornley and is not “above” him either. You may want to check out Gorman’s third selected publication in his staff profile: https://unidirectory.auckland.ac.nz/people/profile/d-gorman
So far, you have produced only innuendo and hot air and not a modicum of hard robust evidence. Talking of “grudges from the past”, do you have an agenda, by any chance?
So you do not dispute that hiring right wingers to positions in health, such as Horn, is say an indirect influence on academia.
Then there is economic ideology and influence on perception of valid public health policy – placing an importance on business activity, thus promoting a health policy that works around that, even if the health outcome is less optimum?
Yeah sure.
Puting the people first, before the economy was not only right – but it would work and possibly lead to political change. Little wonder the right were nervous.
Ignoring those voices saying put the economy before people.
Hopefully the government can take some of the courage in their response into other areas of policy, and thus avoid being accused of being Blairlite.
Yes, I absolutely dispute that the appointment of Horn as Chair of the National Health Board had the influence that you imagine it had because that Board was about the provision and funding of health services. What does this have to do with the latest Plan B brain fart?
Nine years of National-led Government had a perverse effect on NZ academia, especially that wrecker Steven Joyce.
The rest of your comment is just another smokescreen to avoid answering specific questions under this Post.
weirdly, they're not actually offering a plan B in that letter. We haven't had that many lockdowns, so it's hard to know what they are on about. Also, if they believe that income is the biggest determinant of health, where's the call to be raising benefits and minimum wage, and the plan for that?
Yes, and… there is an odd dynamic of denial on all sides about the vaccine. There are risks in rushing to a vaccine, as well as relying on that for something (what?) when we don't know how it will work. Maybe I've missed it (I haven't been following super closely), but I still don't get what the plan is.
Is the vaccine intended to eliminate covid19 like polio? Or is it intended to be like the flu vaccine, something needed to be taken seasonally? Or something in between?
Specifically for New Zealand, how do those questions relate to our closed borders and ideas on when/how we should or could be opening them?
Are we working on the assumption that vaccines are Good, and that we will work out the details as we go along? Not saying that is wrong necessarily, just that I find it odd that we're not really talking about it.
If the idea is that we will be free of covid and able to open our borders in a year or so, I think it’s ok to question how real that is.
https://www.health.govt.nz/our-work/diseases-and-conditions/covid-19-novel-coronavirus/covid-19-response-planning/covid-19-vaccine-planning
what's your point Incognito? The MoH doesn't have a plan yet, and…?
The strategy makes sense, but in the context of my questions it's still a strategy based on best hopes and guesses. Afaik we don't yet know how long the immunity from a vaccine will last, and issues like transmission of the virus by people immunised are still not resolved.
It reminds me of the position re climate change that we can avoid powerdown because soon we will develop the tech for CCS etc. It's a bloody big gamble.
If the point of the vax strategy is to work alongside other strategies like border control, tracing, lockdowns etc, I think that should be explicit. Maybe I'm wrong here, but aren't people expecting we're heading for herd immunity from the vaccines?
What is my point? None, zilch, nada 😉
For the convenience of those who want to find out more information from MoH, I simply provided a link. That is it.
As you can tell from the Menu on the LH side of the MoH webpage, Vaccine Planning is just one of the planks of Response Planning. However, it was always going to be a major plank and even more so now vaccines are starting to be approved and used in general populations, IMHO.
https://www.health.govt.nz/our-work/diseases-and-conditions/covid-19-novel-coronavirus/covid-19-response-planning/covid-19-vaccine-planning#border
Nobody knows how effective these vaccines will be or how long they might last. I think it is safe to say that they are quite safe when they are approved for use in the general population. This doesn’t mean that there won’t be any side effects, some of which could be serious in some rare cases. However, this is carefully monitored; some large clinical trials have been temporarily paused because of reported side effects but this is common practice.
https://www.immune.org.nz/vaccines/vaccine-safety/safety-monitoring
My interpretation of the MoH information is that they aim for ‘herd immunity’, but that they are actively avoiding using this loaded term.
HTH
My interpretation was that they're not aiming for herd immunity at this stage. How did you get to that conclusion from that doc? eg the potential scenarios.
From the last link,
"Vaccine safety is monitored through voluntary reporting of adverse events, passive monitoring, and formal systems that require reporting, active monitoring."
This is inadequate. If you get someone talking about an adverse reaction to a GP, it's up to the GP whether to report it or not, and people concerned about vaccine reactions have been saying for decades that many GPs won't report. This is in the context of anti-anti vaxxer rhetoric and pressure, which is sometimes intense and nasty. GPs aren't immune to those positions either.
Of those situations some, possibly many, will not be related to the vaccination, but the problem with the current situation is it leaves us with simply not knowing. (if someone has the guidelines issued to GPs, I'd be interested to read them. I'd also like to know what the defined period is for mandatory reporting of adverse reactions for new vaccines).
We do know that the MoH is generally useless on disability and chronic illness that it isn't equipped to deal with. We're also seeing it not stepping up on long covid. So it's not hard for those of us already at the sharp end of the stick to be thinking this will be true for people with adverse reactions to the covid vaccine as well.
The position that the vaccine is relatively safe (probably) and will save more lives/disability than not vaccinating (definitely in countries with community transmission, probably in NZ), but who don't address the issues in the health system and assume that things will be fine, are in a position of denial which boils down to a collateral damage position. Understandable, some of us are pushing back against that.
Instead, what we could be doing is saying the vaccine is relatively safe (probably) and will save more lives/disability than not vaccinating (definitely in countries with community transmission, probably in NZ), and there will probably be people who have adverse effects and we shouldn't be afraid of talking about that openly and what it means and how those people will be helped.
Since 'NZ' has purchased more than enough doses of COVID-19 vaccines to vaccinate the entire population, it's likely that all NZers will be (strongly?) encouraged to get vaccinated. But it's also likely that taking a COVID-19 vaccine, like all other vaccines available to NZers, will be a matter of individual choice/responsibility, and I don't expect any NZ government to make all my (difficult) choices for me.
I'll (probably) choose take part in any nationwide COVID-19 vaccination programme (although I certainly won't be volunteering to go first ), and should I suffer a serious adverse effect then (in NZ) I would expect some support/assistance from our over-loaded but still excellent public health services to be available to me.
), and should I suffer a serious adverse effect then (in NZ) I would expect some support/assistance from our over-loaded but still excellent public health services to be available to me.
It's a bit difficult to know where Bolsonaro's coming from with this bizzare list of possible side-effects; why, it's almost sounds like scaremongering.
Cosmetic surgery is a choice; maybe some people will decide to make different choices as a result of the global pandemic; we can only hope.
It's risky waking up each morning – it's even riskier not to. All we can do is educate ourselves about (relative) risks, make the best (informed) decisions possible, and accept there’s no guarantee that we won’t (occasionally) choose poorly.
If by that you mean that you will still be supported to some kind of quality of life, let me disabuse you of that notion. Many people with chronic illnesses get SLP if they're lucky, otherwise the dole from WINZ, they don't get ACC (or if they're eligible for ACC but weren't working in the year before because they were a student or a solo parent or on the dole etc then they get sfa). They get minimal disability support via the health systems because the health system is antiquated around the social realities of disability (eg you might get a few hours of home support per week irrespective of the degree of disability).
If, and that's definitely an if, your disability is a recognised medical condition, you may or may not have trained doctors who know how to help, or there may be no help known, or you may not be able to access the doctors because the ones experienced in your condition are few and far between.
Everything I just said is how the health/welfare/disability systems already operate. I guess there is some chance that covid will prompt some changes to that but given Labour are resistant to ensuring disabled people have a decent standard of living and in fact have no income support policy for them, I'm not hopeful. Also, the MoH has its own set of cultural problems akin to WINZ that that the non-disabled don't want to talk about.
Thanks for that Weka – my expectations in this regard were based on personal experience; I'll have to revise them in light of the information you've supplied.
There are many clues on that webpage that point to it but these are the clearest:
I don’t know any details but my uneducated guess is that the roll-out(s) of vaccine(s) will be monitored with much greater attention and care than usual. I assume that details will become available early next year. However, this appears to be a new development:
In any case:
Obviously, given that NZ roll-out won’t commence before June-21, there will be considerable international experience on safety and effectivity that will guide us here in NZ.
HTH
There are risks in rushing to a vaccine,
It's important to understand how much of the timeframe compression was achieved, because safety checking has not been short-circuited or bypassed.
Almost all of the 11 months since the virus was definitively identified has been taken up by safety and efficacy checking – Moderna's vaccine was apparently developed two days after the genetic sequence of the virus was released.
The speedups have been achieved by steps such as vaccine companies gearing up for production as soon as they had a candidate that might be viable and they knew roughly what production facilities were needed. That's a financial risk for the company (or the government that funded it), but it's not a safety risk. It's also a huge contrast to the usual process of not even thinking about pilot or full production for the next stage until the previous stage is complete and signed off.
The phase 2 and phase 3 trials were also started almost immediately when the information needed for the trials came out from the previous step. It's because all parties involved were closely following the process and doing the analysis and review and giving approval (or not) as fast as reasonably possible. Again, there weren't safety shortcuts taken, it's that everyone involved had a sense of urgency to expedite their part of the process. The comparison to the length of time it normally takes just illustrates how long-winded and needlessly drawn out the normal process is.
Tragically, another reason the vaccine development went so quickly was the way the pandemic massively grew very quickly after the phase 3 trials started. That meant enough trial participants were getting infected soon enough that the required number of infections to get efficacy conclusions happened much more quickly than would have been expected earlier this year. In contrast, other vaccines in recent years have taken much much longer to get results from trials, simply because the disease they protect against is so rare.
I've recently seen a good article that went through all this in depth, but I'm having trouble finding it again. I'll keep looking and post it if I find it.
This isn't the exact one I was thinking of, but it's close:
https://theconversation.com/less-than-a-year-to-develop-a-covid-vaccine-heres-why-you-shouldnt-be-alarmed-150414
Saying "There are risks in rushing to a vaccine" doesn't mean that good things haven't been done in developing the vaccines in shorter time periods. Or that caution was thrown to the wind. It means that even doing our best, there are still potential issues with going so fast. I don't think it's hurts to be honest about that.
OH Gaia now we not only have to cope with Michael Baker's self promoting reaction to every snippit of news . we also have this lot.
They're not "academics" in the accepted meaning of the word.
I don't know who they are but my pick is:
1) They're probably quite young (maybe not) and rather arrogant.
2) They haven't done due diligence on the subject matter because they're right wing ideologists following an agenda to discredit both the government and the main stream academics… of whom they are jealous.
In short, they're nut-bars.
My considered opinion. 😉
Enough of them are employed in academic posts by recognised academic institutions such as University of Auckland and University of Canterbury that a label of academics is accurate enough to be fair. That a few of them aren't academics, but are instead public relations weasels or lawyers or in private practice, doesn't make the description unfair.
From the linked original letter:
However, there is strong evidence for their being ideologically blinded nutbars. That is, one of their first biggest claims, around the timeframe for vaccine availability, has been shown so spectacularly wrong immediately after they wrote their piece. It's not as if the rapid progress on vaccines was any kind of secret, either.
You cannot seriously claim to be giving a considered opinion and also state they are not "academics" when you admit that you don't know who they are.
You seem to have missed the emoticon at more than one level.
Thanks Incog. 🙂
That certainly seems to be an interesting approach.
Does that mean that I can say that some commentator here is a total idiot and is unable to give a reasoned comment on anything at all and make everything OK by putting an "I'm just joking" emoji at the end?
😀
Sorry you are unable to decipher a self-deprecating acknowledgment that my comment was off-the-cuff and lacking any detailed analysis. Perhaps I caught the bug from your esteemed self who is a past master at producing brief, caustic comments with no facts attached.
My response appears to be well backed up by the real experts:
https://www.nzherald.co.nz/nz/covid-19-coronavirus-new-zealand-scientists-critical-of-anti-lockdown-letter-in-top-medical-journal/YL36RS7MHJ7RBXUO572SXV53PM/
I'm not really sure that the people in the article you link to are disinterested individuals. They are, after all, people who pushed for the total shutdown approach.
Michael Baker was one who said that there could be about 80,000 deaths in the absence of a lockdown. Such a scenario never happened in any country. Even Sweden has only had about 8,000 deaths in a population that is twice that of New Zealand
He also said we didn't have to worry about mutations of the virus.
'Baker said he wasn't worried about the virus mutating further as it spread across the globe.
"These viruses are under huge selective pressure and generally the selection is towards variance that is more infectious and less lethal.
"So what we might tend to see over time is the virus will become part of our normal bugs that infect our respiratory tract like the other four coronaviruses."'
I wonder if he still thinks that, and whether there was any peer review of his own work back in March? I once emailed him to ask about peer review of his predictions. I never received an answer but even if he saw it I doubt if he would have had time to waste in answering a random question from someone he would never have heard about and who certainly doesn't have any medical background.
https://www.rnz.co.nz/news/national/412734/covid-19-lockdown-critical-people-change-behaviour-expert
I think we could follow the example of Taiwan which never had a total lockdown and who kept their schools running. Total of 7 deaths in about 24 million people the last time I looked.
Thanks for sharing your opinion Alwyn. NZ’s not perfect, but the last time I llooked our team was doing OK too, so credit where credit's due IMHO.
Except for the bit in february where they postponed the opening of schools for two weeks. Banned cruise ships from 6 feb. Most foreign nationals by March.
So, yeah, they got in even earlier than us. We made the finals, they're on the podium.
That doesn't make the plan B crowd anything other than a festering pile of bullshit, though.
This is misleading on more than one account. I think you’re referring to this: https://www.stuff.co.nz/national/health/coronavirus/120604818/new-model-shows-coronavirus-could-kill-80000-kiwis-without-lockdown. However, Professor Baker was not involved and he was not an author on that paper. However, that model was adapted from a model developed by Baker and colleagues – Baker’s model predictions never went as high as 80,000 and only (!) as high as 10,983, about which they said:
https://www.health.govt.nz/system/files/documents/publications/report_for_moh_-_age-specific_impacts_covid-19_pandemic_final.pdf
The other misleading aspect of your comment is that you are hung up on the exact number of 80,000 rather than the implications of not doing anything, which would overwhelm the NZ Hospital system and lead to high numbers of deaths. With your training in Economics, you would know that all models are wrong but that some are useful.
The third misleading aspect is that models were adapted as more information and data came in. Of course, this lowered the estimates for the number of deaths in New Zealand. This is how good science works. Anyway, you may want to read the NOTE on page 1 of Baker’s paper.
My confident guess is ‘yes’, why would he not?
See comments above.
You seem to have a fondness of bringing Taiwan into the conversation even when this is mentioned at all in the OP. Funnily enough, New Zealand has changed its response over time to resemble Taiwan’s, for obvious reasons. The World can learn much from Taiwan and New Zealand’s response to the pandemic:
Potential lessons from the Taiwan and New Zealand health responses to the COVID-19 pandemic https://www.thelancet.com/journals/lanwpc/article/PIIS2666-6065(20)30044-4
If you have anything specific in mind, perhaps you could enlighten us? Or do you mean to say that we could have followed the example of Taiwan from the outset? Maybe you should e-mail the Plan B activists because they’re stuck in Sweden still.
The material I was quoting from was in the link I posted with my comment. It was from RNZ and not Stuff as you surmise.
If you look at my link you can see the sentence directly before, and the ones immediately after the photo of Professor Baker.
'"It's so critical in this period that people change their behaviour and not share this virus."
Recent modelling predicted the lockdown could save about 80,000 lives across New Zealand. Dr Baker said large-scale testing, contact-tracing ability, and tighter border control systems were needed to contain the illness.'
That sounds that Dr Baker agreed with the 80,000 estimate doesn't it?
Of course, he [Baker] agreed with the conclusions and implications of the study by Hendy and colleagues, as it was based on his own work! That was never in question, was it? But now you are moving the goalposts again, from “Baker said” to “Baker agrees”. It seems to me that you’re on one of your pedantic point-scoring hunts again. Just as well, it takes one to recognise one, which is why you and I get on so well here.
In any case, that was March, and Hendy and Baker have moved on, as intelligent people tend to do, unlike you and the Plan B rabble, who seem to be still stuck in Taiwan and Sweden, respectively, and unable to join in a reasoned debate about the future.
Terrible that Baker should have overestimated the risk. It may only have been 8,000 deaths. One in everey 500 kiwis or so. That would have changed everything …
I am curious Micky.
Where do you get the numbers from that you use in this calculation? I could have understood if you had used a number like that of Sweden, which is about 1 in 1,250 but your chosen value is about 2.5 times that. Why did you pick that value.
Incidentally you could assume that we had done well, and achieved results like those of Taiwan. Our death rate was, allowing for the different population and the number of deaths in each country, about 17 times theirs. Of course they went hard and early rather than carrying out the rather dithering approach we seem to have followed.
Another of your idiosyncratic ‘querying’ comments that are so typical of a pendant with training in Economics, i.e. hung up on numbers 😉
Are you, by any chance, a Plan C activist bringing up Taiwan in every conversation about Covid? I wonder who funds you …
Heh, "pendant". It works. Given the load of swinging bollocks you responded to.
@andre..
what actually was incorrect/'bollocks' in what alwyn said..?
I see no sign of testicles in his words..
You’ll need to use a stroboscope.
"I wonder who funds you …"
Nobody old chap except I suppose my wife who lets me waste my time in reading and commenting on blogs.
Isn't such a statement by you a breach of the sites privacy rules? Or is it valid for me to wonder the same thing about you?
I’m just a lune wolf roaming TS for easy prey when I’m hungry.
@incognito
as taiwan has done better than anyone else..of course they should feature in any covid conversation..
also helps to stem our national propensity for self-congratulation/smugness..
Are you sure about that? By what measure(s)? Don’t give us your reckons, give us a link.
But her e-mails …
‘kay, this is by far the worst thing that could happen to us and needs to be fought to the death. The winner must not be smug about it. FFS, I thought we got rid of Sir John Key!
Taiwan's response is great and everything but how about comparing apples with apples. For instance, do we in New Zealand have a mask-wearing culture? No, we don't.
I replied to Alwyn yesterday with a very informative and educational link to a recent article in The Lancet about Taiwan and New Zealand in the context of Covid-19. If he had read it and taken it in he would not make the comments he’s making, IMHO.
Alwyn, you weren’t always so keen on Taiwan – first there was South Korea, although we probably shouldn’t emulate them since their 'COVID deaths per million' has sadly climbed to more than three times NZ's.
But you think you know where NZ went wrong; such a team player
The distance between South Korea and Taiwan is about as short as between Auckland and Balclutha but Cook Strait is swimmable and the East China Sea is not 😉
We need more loyalty in this day and age!
I misread your statement Alwyn. Correct figure would be more like 4,000 or very roughly one in a thousand kiwis. Still to many …
I think charlatans is the best description.
Academics offering uniformed opinions outside their areas of expertise.
Some of them are lawyers and PR folk, of whom truth is not expected. But the medical professionals may need their credentials reviewed, in the interests of patient safety.
A measure, albeit a fairly coarse one, of scientific impact of an individual is how often their work is cited, which can be looked up easily enough on the Web of Science if you have access to a subscription.
The total citation counts of the two most recognized members of Plan B are Schofield (citation count = 5054) and Thornley (total = 1341).
In comparison, the counts for the three most visible supporters of Plan A are Baker (5313), Wiles (2225) and Hendy (1394).
So at least based on the available data, I don't think that you can just trash the credentials of the Plan B team in that way. You can disagree with them (as I do), or question their motivation, but you cannot use this argument to claim that they are not qualified to contribute to the debate or are somehow less qualified either.
you cannot use this argument to claim that they are not qualified to contribute to the debate or are somehow less qualified either
If they insist on assertions that are patently untrue, as Baker points out, things like
when NZ has bought two already they discredit themselves.
Here's the full paragraph,
I think it's pretty clear there that the 'may never eventuate' sentence is in the context of eradicating covid19. Or in the wider context of the article, elimination for NZ.
This is a reasonable position (that an effective vaccine in terms of elimination or eradication may never eventuate). See my comment elsewhere in the thread on what's the actual plan for NZ.
It's worth reading the whole piece. I disagree with their basic premise (and lack of an alternative plan), but the issues they raise aren't meaningless.
https://www.publish.csiro.au/HC/pdf/HC20132
The issues they raise might not be meaningless in an absolute sense, but it's farting against a thunderstorm.
Who seriously cares, at this point in time, whether covid19 is reduced to rabies or tetanus? Endemic in some areas, particularly in wild hosts, but you get a shot before travelling to those areas. Big whoop compared to a million dead inside a year (and that's the official count – comparing official counts with excess mortality seems to not tally up).
Yes, they are issue that will need examination eventually. But I'm pretty damned sure the only reason plan B are bringing up polio is because they value international passenger dollars over people dying right now.
Sure, but isn't the point of mass vaccination in NZ so we can save the economy?
I've seen pro-vax people using the polio argument in the other direction and it's daft then too.
Not sure what you second paragraph is about. They're not arguing against vaccination.
As for who cares, I do. Some people are good with the 'trust us we know what we are doing' approach from the MoH and don't want to talk about the problems with that, there are many with direct personal experience who cannot afford to do that.
As someone in a grey area personally on safety re both covid and vaccination, it also matters to me what NZ is intending to do. Are we intending to let the virus become endemic here at some point like flu? Why are we not having an open conversation about this?
Plan B's position is pretty clear, I've said I don't agree with it. What I don't get is why we're in such a false binary in terms of looking at all the issues.
The point of mass vaccination against covid is to save lives. If some economic sociopaths think that coincides with their concept that the only thing worth preserving is GDP, well that's a happy coincidence.
The second paragraph is because they are actually arguing that global elimination via vaccination is an impossible (or at least unrealistically long) goal, in order to belittle short term efforts to (checks notes) save lives.
The intent is to eliminate. An effective vaccine and no reservoir in the wild would make that possible. If someone turned up at an airport with active polio, dollars to doughnuts we'd be vaccinating anyone who even vaguely came into contact with them, to eliminate it again. NZ does not take infectious diseases lightly.
We don't do that so much with the flu because elimination of the disease itself is likely impossible at this stage of tech. But we don't know that covid is like that. If the best we can do with covid is what we do with the flu (assess the most likely strains this year, do a vaccine for each one). But that is the real "plan B", and not anything close to the ideal. That's not high on the discussion list at the moment, because quite frankly anybody who is anybody is focused on stopping the damned pandemic.
Whether that means vaxxing it down to low levels like influenza or elimination depends on multiple variables to which nobody yet knows the answer – vaccine effectiveness long term, the rate of the virus mutations that take it out of the vaccine envelope, and so on. If a single jab lasts ten years and takes out ~all variants, we're golden. If not, that's the hand we're dealt.
This podcast from JAMA goes into some depth about how vaccination strategies may impact on herd immunity. It's in the second half of the podcast- the first relates to how to prioritise populations for vaccination in a US context.
Interestingly the candidate COVID vaccines are all effective at preventing the development of severe disease, but the impact on transmission by vaccinated individuals is not yet apparent. Polio, influenza and measles vaccines are really effective at preventing transmission, whereas pneumococcus vaccination, for example, doesn't prevent the bacteria circulating in the community, but does prevent serious disease in the vaccinated individual.
Interesting figure of >100% population vaccination rates is mentioned to the astonishment of the interviewer!
https://edhub.ama-assn.org/jn-learning/audio-player/18570273
also, the comment you replied to was me replying to Stuart because he's selectively quoting in order to undermine the people. I think that's sloppy and detracts from being able to address the issues raised by Plan B. The whole 'they're not real academics' lines in this conversation are pretty low level responses, that won't serve us in the long run.
I agree they're academics. But they're sloppy academics pushing a barrel of shit. Why their letters got published, I have no idea. Frankly I think it was clickbait by the publishers.
It is indeed worth reading the whole thing. The assertions are troubling, and many or most of the arguments are economics rather than science based.
The NZ government and the majority of its health experts have maintained their advocacy for elimination, in spite of:
– a vaccine being at best a four-year wait;
So, not 37 years but four years now? At best this shows a serious lack of imagination – at best the vaccines we have arranged for will rollout mid 2021, and prove reasonably effective. Should they prove inadequate there are a number of others in development – rather more than usual as a result of the grave situation many countries are in.
The problem I have here is you now intentionally taking sound bites from the letter and using it to support your position of antagonism against them, presumably because you don't like what they are saying and believe it's better to undermine them than to argue against what they are saying.
Their meaning on this point (elimination in NZ) is clear enough and is supported by evidence (see Incog's link above to the MoH strategy doc): we don't know yet how covid vaccination programmes will work, and we don't know when/if we will get a vaccine that enables elimination/eradication in the NZ context.
If you think the 2021 roll out of the vaccines that NZ has access to are going to enable elimination of covid in NZ, please explain how. What I can see is vaccines that will be used alongside our current strategies, not replacing them.
Your faith in the development of an eventual vaccine that allows elimination is no more valid than their concerns that there won't be one or it will take a number of years. As I’ve said, I disagree with where they go after that, but the denial on the other side of the limits of the vaccination programmes doesn’t help.
and believe it's better to undermine them than to argue against what they are saying.
Yup; the gross politicisation of this disease event has proven even more deplorable than the same forces that played out with climate change.
Your faith in the development of an eventual vaccine
Is neither here nor there. The writers asserted that the best case for a vaccine was a working one within four years. On the contrary, a best case admits the possibility of some of the existing vaccines working as well as the trials of them to date suggest, i.e. reasonably well. This is the only position for which actual evidence exists to date. It may not work out as happily, but to assert that it cannot without any evidence is going too far. Inventing an outcome to support a stance critical of the government is a shameful retreat from any pretense of academic standards, bringing both the authors and the publication into disrepute.
The letter was received dated 5th November, and I think we can assume was written at least some weeks before this. The delivery of new vaccines is very much a moving feast, and only recently this past month have promising trials been announced.
At present there are four leading contenders; the Pfizer mRNA version that is being currently rolled out. Problems here include the need to store at -70degC, the need for two doses, and the fact that vaccines are nowhere near Pfizer's core business. It will likely be useful for medical people and other high priority candidates in the next few months.
Moderna have been in the vaccine business for a while and are ramping their mRNA version up fast. Like Pfizer they need two shots, but the distribution only requires conventional freezer temps around -20degC. Both of these are good news as being available now, but probably aren't the global solution we need.
Oxford trials have been a bit messed up with some mistakes in dosing, which is going to delay it's roll out. It's not the mRNA type the first two and uses fairly conventional low cost manufacturing methods and requires only normal refrigeration. In six months time it should be outselling the first two.
Perhaps most interesting of the four is the Johnson and Johnson approach which requires only one dose, no onerous storage requirements and is relatively low cost. It looks like it will come online about March, and can likely piggyback on the distribution chains already established by the other ones. Any doctor or health clinic anywhere will be able to administer it. This is the one that will make or break the vaccine approach to ending COVID globally.
If at least one of these four vaccines can be successfully rolled out over the northern hemisphere summer, then it's likely a third winter wave will be prevented.
I'm not a big fan of relying wholly on vaccines to end this; mainly because it allows us to bypass the obvious questions as to why it's the developed Western nations in North America and Europe who've been most vulnerable and avoids addressing issues around poor underlying health, highly prevalent co-morbidities, Vitamin D deficiency, and much more.
But pragmatically I accept this is what we're being conditioned by the media and health authorities to accept as 'good science', and objecting is going to be like farting into a hurricane.
There are other vaccines in development, so that failing our existing options working, we're not back at square one.
Some scepticism of vaccination as a solution to viral infections may not be misplaced – but the fact is that this article is a deliberate rhetorical assault on the government's handling of Covid, and on lockdowns should the need for them arise again. Real scientists eschew rhetoric – it is no substitute for data.
Lockdowns have enjoyed mixed success around the world, but they have been reasonably effective in NZ, presumably because of limited infection paths and (now) a decent tracing set up. I am sure the MoH would prefer not to use lockdowns again, but the idea that they could be taken off the table by a couple of persons who have no coherent alternative proposal is about as sound as Gnat economic policy.
As Sanctuary notes, this was a bad faith piece, and need not be humored.
And a fair bit of the response on this thread hasn't demonstrated much better degrees of 'good faith' either.
Don't worry RL, once this global pandemic is under control (the number of "Currently Infected Patients" has just topped 22 million, up from 7.8 million on 3 Oct.) then there may be time to draw breath and ask those obvious questions. In fact, they're so obvious that some are asking them even now.
Maybe they should have also fact-checked that claim about a multi-billion dollar market.
We're on the same page, not wanting to put all our eggs in one basket
And a fair bit of the response on this thread hasn't demonstrated much better degrees of 'good faith' either.
Oh rubbish – these clowns have gone way beyond their scholarly mandate for a cheap shot at the local response. A cheap shot so jaded its manifest shortcomings make it absurd within scant months of publication.
The fact is the authors have been living consequence free for too long, and figure that that can dress up nakedly politicized bullshit as informed dissent. All that they have demonstrated is that they are not informed.
One hopes so! BTW, if you go https://euromomo.eu/graphs-and-maps/#z-scores-by-country you’ll see that some countries have experienced a mini-wave in their summer and these countries are now in their third wave of daily new cases & deaths 🙁
Re the obvious question of why it's some "developed Western nations in North America and Europe who've been most vulnerable", part of the answer could be poor leadership. But when I asked a Belgian friend why they have by far the most COVID deaths per million of any country (1,650), she replied "Belgians don't like being told what to do."
Food for thought, IMO. Maybe NZers recognised how vulnerable we’d be if COVID really took hold here, and that COVID is an 'enemy' best fought by following the consensus advice of health experts – kudos to the team/flock of nearly five million. We don’t know how lucky we are.
I was following Plan B in the beginning because I thought that they actually had some good points to make and to be perfectly honest I still think so, more than I care to admit here.
However, I think they were ill prepared and stumbled, at both the science and PR levels. They teamed up with Blackland PR, possibly for the right reasons, but failed to get much traction mostly because they were up against it.
I also think they made a classical mistake of being wedded a little too much to their own ideas and message and didn’t take criticism well, whether fair or unfair.
If you decide to go against the ‘establishment’ and general opinion, you must ensure to be near flawless, resilient, act with unbreakable & unbendable integrity, and have a damn strong argument and an even stronger unwavering communicator. I think they failed on all these counts to some degree.
Just as the National Party, Plan B became more reactive, reflexive & defensive, and antagonistic instead of constructive and this became a vicious circle. They were definitely not the only ones in the World who spoke up and against the prevailing ‘orthodoxy’, but as others such as John Ioannidis and Anders Tegnell or even the nation of Sweden, for example, can attest this was not for the fainthearted. Of course, politicians such as Trump and Johnson were never far away, muddying the waters, turning clear fresh water into murky swamps.
Plan B have done both the public and scientific debate a huge disservice, in my view. We need to have these debates for good reasons. It takes a lot of guts to front up in public but they have raised the barrier even further 🙁
All my personal opinion, as per usual.
Pretty much.
If covid was significantly less infectious or less lethal, it's possible that the economic hit would cause more harm than the protective effects iof shutting everything down for weeks on end. And I'm pretty sure that nobody expected a recovery to be so quick, and stronger than for those nations just "living with" the virus.
So the govt had them on one side, and Baker and co on the other saying "lock it all down now". Fair call, we got lucky and the govt made the right choice in a messy information environment.
But to still be pushing it now? faaaarkk
thanks Incog, that's solid analysis, which I pretty much agree with (although haven't followed Plan B as closely).
The other issue in this thread is to what extent we can have meaningful discussion about various issues that don't fit the dominant NZ narrative on covid, and where they overlap with organisations like Plan B. Rather than knee jerk reactivity that writes the issues off along with writing off Plan B. Always appreciative of those that will dig deeper (and there's been both in this thread).
"…It's worth reading the whole piece. I disagree with their basic premise (and lack of an alternative plan), but the issues they raise aren't meaningless…."
Only an idiot would suppose these people are arguing in good faith, and the response has to be calibrated within that context.
What does that have to do with what I said? If you want to ignore the issues, go ahead /shrug.
Hendy only has 1394 citations? I find that hard to believe, but without a subscription to Web of Science, how can we tell if you speak the truth?
The raw number of citations is as useful as the IQ of your mother-in-law.
In any case, here we have a herd of academics who are trying to influence public opinion and health policy and as such, their intended impact goes well beyond the boundaries of research or scientific impact.
https://scholar.google.com/citations?user=RHyTIvMAAAAJ&hl=en 2038 citations of Hendy
https://scholar.google.com/citations?hl=en&user=ji2WVyQAAAAJ 2119 citations of Thornley
At least Google Scholar is a source, with all its drawbacks, that we can all read without subscription.
Academic credentials mean nothing if their bearers don’t apply the rigour of academic standards to their propaganda pieces. It is like an F1 driver crawling behind the wheel of a Corolla and driving while 8 times over the limit and not wearing a seatbelt.
Re: 'I find that hard to believe, but without a subscription to Web of Science, how can we tell if you speak the truth?'.
If you are going to accuse me of being untruthful then you might want to get your facts checked first. You could ask anyone studying or working at any major university to check it for you. All the main universities in NZ subscribe to the Web of Science.
My comment was a legitimate response to the claim that 'They're not "academics" in the accepted meaning of the word.'. I still stand by my response. We might not agree with them but it is simply dishonest to pretend that they are not real academics either. And just for the record, the ability of an academic to cultivate the media well and get extensive media coverage for themselves can be quite independent of their scientific impact or standing.
Tsss, so defensive! I said that I cannot check if you speak the truth without a subscription. Your ‘helpful’ suggestion to find somebody in a NZ university is anything but helpful at this moment in time. You asserted the facts and the onus is on you to show us that they are correct and true or convince us that we should take your word for it. How do I know that you’re not one of Plan B activists, for example? Can’t you see the dilemma here?
For my ‘fact-checking’, I used Google Scholar and the numbers appear quite different from yours!?
Of course, you do, because you missed the whole point, which is that they do not perform as rightful academics. This is a point made by Professor Baker too.
On this, we agree. In fact, I said as much when I mentioned “impact” 🙂
Any reader of this blog at any university can check my data and are welcome to do so. I don't see any need to respond beyond that to this point. However, there are simple reasons as to why Google Scholar citation counts are always higher than Web of Science (or Scopus) counts.
First (and most importantly), the Web of Science only counts citations of ones work in peer reviewed journals. Google Scholar counts citations of ones work in pretty much everything that it can find on the web, including not just in peer reviewed journals, but also in non peer reviewed work, reports, blogs, etc. For this simple reason Google Scholar counts are usually about 1.5x those of Web of Science counts, as indeed your own data is relative to mine.
Second, Google Scholar can be gamed. The academic sets up their own Google Scholar page and controls it. There are ways that it can be gamed to inflate ones citation count and there are very good reasons why universities wont normally use Google Scholar counts for staff promotion.
I could not use Google Scholar counts in this case for the simple reason that Baker has not set up a Google Scholar profile, and as Baker is a key player here, it was necessary to use something else (e.g., Web of Science) to allow for a fair comparison.
‘kay, still shifting the onus to somebody else 🙁
Raw citation counts are a meaningless metric at the best of times, anyway.
If Google Scholar also counts citations in non-peer-reviewed media, it might actually be a better metric in this context than that Web of Science one for which you have to pay.
I hope that you’re not so naive to believe that Web of Science cannot be gamed in some ways, but I take your point that it is important to compare fruit with fruit when possible.
This whole thread is a bit moot, IMHO.
You’ll have to ask the Editor but one presumes she deemed it of sufficient interest and importance to the journal’s readership to let this poor propaganda piece pass for publication in her journal.
The take-home message is, for me, that if you have a point to make, make it as well as you can and start a proper debate based on good faith. The Plan B activists failed on that count, again, and again. I’ve called them out here for acting as pseudo-scientists and they are continuing with their charade.
It is definitely funded by fresh water (chicago) economic commandments. The smell of the taxpayers union is pervasive.
I accept that both academics and politicians are strongly egotistical but why the anonymity?
Academics, like politicians crave public attention (at least) among peers. This effort seems pointless.
Sideline experts telling the ref what to do.
Well, show us your evidence then.
Well I wonder if these fucks are enjoying their holidays rather than being told to stay at home in a quasi-lockdown lockdown using their holidays to quell surge and having to spend 8 months and the forseeable future wearing masks, social distancing, feeling guilty about seeing family and friends and feeling vulnerable at all times.
Fuck them. And fuck their backers. NZ people already showed how they feel about people peddling BS about the pandemic. Long may they continue. Most people in the world would be grateful to be in NZ now.
We need to see this Plan B letter for what it is – not good faith science but a planned piece of propaganda from BlacklandPR whose release was designed to fill the news void around Xmas. Luckily, its central thrust since submission for publication was made nonsense by the rapidity of the vaccine development, but it doesn't mean whoever is funding these Plan B clowns won't try again.
Wonder if these clowns have links to the ACT Party – or somebody rich who has links to the ACT Party.
If you mean by "these clowns" Blackland PR's Directors etc, once again you should check who you are talking about before hitting your keyboard.
If you had done so, with your long association with the Labour Party, I would be surprised if you (and MickySavage) did not recognise the name of one of the Directors of the company – Mark Blackham – listed in the Covid Plan B letter.
Why? Because Blackham was Press Secretary to Mike Moore back in the 1990s, ie from the About Us section of the Company's website https://blacklandpr.com/about-us/
The other Director, Nick Gowland, also worked in the Beehive for Helen Clark's government:
Blackland's two PR Consultants, Ben Craven and Dylan Lee, also have had considerable experience in Parliament and government
After graduating from Massey University with a Bachelor of Communication, Dylan worked for Select Committee Services in the Office of the Clerk at Parliament where he developed knowledge of Parliamentary policy and procedure.
The website also shows that Blackland PR carries out MP career research and publishes it on their website (well worth looking at IMO – https://blacklandpr.com/mp-career-research/
The survey has been conducted within a few months of each new Parliament since 2014.
The only mention of the ACT party I could find was that Blackland PR selected their Communicator of the Year awards with Nicole McKee, the new ACT party MP as the 2020 recipient of the Blackland Communicator of the Year award . with Greg O'Connor, Mike King, Sir Peter Gluckman , and Shamuveel Equib previous recipients of the award. https://blacklandpr.com/communicator-of-the-year/
This para should also have benn in quotes but edit time ran out
Don't know what all that has to do with the price of fish.
I was replying to Sanctuary who used the descriptive word "clowns'. Imo it is well placed in this instance.
"…The only mention of the ACT party…"
Given the homogenity of neoliberal & libertarian ideology in our political & managerial elites, particularly in the Moore/Clark era it should not be a surprise that members of the political and managerial classes can move smoothly through a revolving door between private and public PR.
The main consideration is defense of the extreme centre and neoliberal hegemony, not any particular set of moral values – although I am sure the various associates of Blackland dutifully take granny a Xmas present in her rest home and possibly even give to charities who support the immune impaired – it is just such personal considerations are never allowed to interfere with the cool professional need to lobby on behalf of those who regard granny and the immune impaired as expendable.
The Plan B crowd had organised a Symposium on Parliament grounds that was sponsored by David Seymour. Check out the Programme @ 4:10 PM.
https://www.covidplanb.co.nz/wp-content/uploads/2020/08/17-august-webinar-programme.pdf
Also the GDP figures must have been a real shock …
Further to these yo-yo's and their reckons, this is from Mediawatch and their round-up of the years goings on, ala Covid.
Warning! Contains excerpts of Hoskings, but only to highlight his, and his colleagues, rank hypocrisy.
https://www.rnz.co.nz/national/programmes/mediawatch/audio/2018777800/2020-hindsight-media-in-the-year-of-covid-19
I am still pointing out to people, who use the word lucky to describe the situation we are now in, that it is not luck. It is good advice, well communicated and then trusted and followed by the populace.
As for the title to of the OP, that NZ could be like Sweden.
Well cases numbers are one thing, the deaths (which are a good proxy for serious illness as well) are quite another.
The selective misuse of data just irks me beyond all belief. Sweden for instance may well have had a quite large second wave of case numbers as the OP highlights, yet remarkably (as with most other places) the death rate of this same wave has been much lower, and is now dropping away to almost zero again. The Swedish response may not have been ideal, but neither is it exactly the insane catastrophe some people want to paint it as.
I'm clearly on record as saying that the lockdowns and isolations were the correct response at the beginning when we really didn't know what the potential of this virus was. But now it's 10 months later and we now know one hell of a lot more (and probably have a fair bit more to understand) about COVID, and I think it's perfectly reasonable to at least talk about more nuanced, intelligent paths forward.
Politically the calculus of the current ideology is 'either you submit to a medical procedure (a vaccine), or we will control your freedom of movement'. The team of 5 million may not have an unlimited appetite for such a draconian response to a disease that's definitely worse than seasonal flu, but as time goes on it's becoming clear it's not the major catastrophe it could have been.
Meh.
Apart from being a bit slow off the mark right at the start of the pandemic, I reckon the government response has been very reasonable and struck a good balance between maintaining as much freedom as possible while keeping public health at a reasonable high. Turns out to have been a good strategy economically as well. So I'm very happy with the decisions made so far, and what is being said about the ever-evolving near future.
Looking ahead, I like the idea that anyone wanting to come here from overseas needs to have been vaccinated with acceptable proof at least two weeks before travel (or have good medical reasons not to be vaccinated). If any citizens want to return without getting vaccinated (and don't have good medical reason not to be vaccinated), they can spend two weeks in managed isolation at their expense. Fuck 'em, we don't need to make it easy for antisocial arseholes to come here and spread disease.
As far as internal freedom of movement, I have not seen any proposals for compulsory vaccinations, nor proposals for movement restrictions on vaccine refusers. I'm good with that. But I wouldn't be happy about the borders getting opened up until everyone in NZ that wants to be vaccinated has received it.
There is still a long way to go on the vaccine front; assuming it's going to be the silver bullet (like it was for smallpox) is a tad optimistic even by my standards.
That’s why it’s worth at least talking about more nuanced, less draconian responses.
I agree but only to a point. The media has been unrelentless in exaggerating Sweden as a disaster. In fact its per capita death rate by Covid is 25th globally, still pretty terrible, but the US and UK and much of Latin America are much worse. There are however two reasons why copying Sweden would result in a much, much worse disaster here than it is in Sweden. Both are based on the fact that NZ has much more inequality in Sweden and that in Sweden the rich pay their fair share of tax:
1. Sweden (through its higher taxation of the wealthy and of property) has simply invested much more in its public health system than has NZ, and they therefore have a much better capacity to deal with a covid outbreak. Yet then there intensive care units are full to capacity. NZ's health system simply couldn't cope with similar numbers.
2. NZ has much more systemic poverty than Sweden, and therefore a much higher incidence of diseases resulting from poor diet like obesity, heart disease and diabetes. These diseases greatly increase the risk of serious illness and death for those who do catch Covid.
As you know, the media like to over-hype things in both directions.
If you click on this link (https://euromomo.eu/graphs-and-maps/#z-scores-by-country) and select just the four Scandinavian countries (Denmark, Finland, Norway, and Sweden) and start the time-scale at 2015-01, you’ll see that the mortality patterns in the four countries have been strikingly similar since 2015 or since inter-country comparisons were possible until Sweden became an ‘outlier’ due to Covid. There are many countries that fared worse but Sweden could have done better, much better too. The sad thing is that Sweden, like many other countries, had a distinct second wave of deaths, which could have been minimised, at least, if they had changed their ways based on the information and knowledge gleaned since. So, to portray Sweden as some example that we should follow is somewhat ‘challenging’ in light of these (and other) facts, which is a point raised in the OP.
I don’t think it is right to put vaccination against curbing of freedom of movement as a dichotomy and that both are likely to operate simultaneously (in concert) for at least some time.
I don’t know what “draconian response” you have in mind but almost all of the people in New Zealand were able to celebrate Christmas in complete freedom. Except for a few PS5s not arriving on time (https://www.stuff.co.nz/entertainment/games/123374490/playstation-5-selling-on-trade-me-and-facebook-for-more-than-twice-the-retail-price), possibly caused by Covid measures, things are not too bad here.
Some fortunate Kiwis have not been able to go off on their overseas holidays and they may feel a ‘little annoyed’ but they don’t comprise “the team of 5 million”, only a small-ish fraction, and they can now sink their hard-earned money into luxury cars (https://www.newshub.co.nz/home/money/2020/12/luxury-cars-prove-popular-alternatives-to-international-travel-as-sales-soar-over-last-six-months.html), renos (https://www.stuff.co.nz/life-style/homed/real-estate/123800232/reno-boom-bites-tradies-in-short-supply), and buying new houses (https://www.stuff.co.nz/life-style/homed/housing-affordability/123799660/kiwis-splash-out-12b-more-in-house-buying-frenzy-this-year).
One issue that needs urgent attention, IMO, is compassionate exemptions.
There's rightly a lot of focus on Sweden because they insisted on a relaxed approach which didn't impinge on people's personal freedoms and business activities. People’s health came second. Swedens approach was used as a stick with which to beat the New Zealand's government with.
Turns out Sweden fucked up royally and it's only right to keep pointing that out.
Turns out Sweden fucked up royally and it's only right to keep pointing that out.
Dead right.
"I believe we have failed. We have a large number who have died and that is terrible. It’s something we all share the suffering from," King Carl XVI Gustaf said in a Christmas interview with Swedish broadcaster SVT.
Dunno RL looks like Sweden's deaths are peaking now.
https://ig.ft.com/coronavirus-chart/?areas=usa&areas=gbr&areas=swe&areasRegional=usny&areasRegional=usnj&areasRegional=usia&areasRegional=usca&areasRegional=usnd&areasRegional=ussd&cumulative=0&logScale=1&per100K=0&startDate=2020-09-01&values=deaths
I am also interested in the ongoing health problems like increased susceptibility to strokes. I don't think we are overestimating the effects of this virus.
Try the graph I linked to above. Worldometer has the daily death rate trending right back to low numbers, and the entire second wave a fair bit smaller than the first.
https://www.worldometers.info/coronavirus/country/sweden/
Be wary of trying to work out a trend in the last few weeks of data for Sweden. Their data is by date of death, and they can take a long time to confirm a death and report it. So they always look like they are trending down over the last few weeks, but the data for any given date can get adjusted upwards for weeks as more reports come in. Over the holiday period their reporting is likely to be delayed as well.
Other european countries present their data by date of report and that doesn't change afterwards.
https://ourworldindata.org/covid-sweden-death-reporting
Given that the daily death rate peaked on Nov 29 and has been falling since, it looks like the Swedes are now 30 days behind on their reporting. Or maybe not …
Maybe you're looking at a cached version? I just checked worldometer and their recent peak deaths are shown as being around December 6 (single day and 7-day rolling average), or December 4 (3 day rolling average).
Just outta curiosity, do you ever sleep?
I thought Sweden was reasonably up-to-date with their reporting: https://www.worldometers.info/coronavirus/country/sweden/
If you click on the corresponding source link (https://experience.arcgis.com/experience/09f821667ce64bf7be6f9f87457ed9aa/page/page_0/), you’ll see that most recent update was 22 Dec. According to that webpage, they do an update every Tuesday-Friday at 2:00 PM. I assume that with Christmas there is a slight delay in reporting and testing numbers may also be a little lower.
The ourworldindata link explains it thus:
So yes, they are reporting their info regularly. It's just that each daily update can (and usually does) look back to increase previously reported daily totals.
So what it means for chart-watchers is a daily update can change the shape of the curve going quite a way back. The alternative of just using the date of report means the past shape of the chart won't ever change, but the reported data becomes somewhat more of a lagging indicator. What really needs to change (for data obsessives, anyway) is for Sweden to crack the whip and improve the reporting so the info comes through in a much more timely manner.
Ah, that’s useful info, thanks. IIRC, Sweden changed their reporting significantly a while back but I cannot remember the reasoning for that at the time.
This is a very recent and excellent commentary in The Lancet:
COVID-19 and the Swedish enigma (https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)32750-1/fulltext)
It echoes one of my (too many) comments (i.e. @ 13.3) under this Post yesterday:
However, rather than bashing Sweden for its relatively poor performance so far, there is a lot to learn from them and we shouldn’t be so smug and pretend we have nothing to learn in this context.
The commentary raises many areas and action for improvement of response that are definitely not specific or unique to the Swedish situation.
To highlight a few, also because they touch on issues raised by weka, mainly:
So, instead of watch & weep it must be listen & learn.
That Lancet article is helpful. One point that did leap out to me is this:
Not being much informed about the Swedish health system I found that quite surprising. It's a factor they have in common with the USA who have also been an outlier example. .
And as you say, there has been plenty of exaggeration of the Swedish case on all sides; when in reality they've just not done particularly well. But then again so have plenty of other countries ….
As far as I can see Baker and the plan B lot are just slightly different hues of the same color.
What they both are saying is "we should be doing something (undefined) different to what we are doing"
Baker has so far contributed ziltch to the discourse. he is simply engaged in self promotion. He does not like plan B because it takes the spotlight off him!
Is that the only reason that Baker “does not like plan B", do you think xanthe?
Same goes for Wiles, Hendy and Dickinson, do you think?
No and No
You may think it clever to put up straw arguments and then shoot them down. I do not. Its kinda a dickhead strategy
Thanks. – more than enough dickhead strategies to go around I reckon
An interesting opinion on which we’ll have to agree to disagree.
“Each year the PHA honours individuals or groups for their outstanding contribution to public health action by naming them Public Health Champion for the year.”
https://www.nzdoctor.co.nz/article/undoctored/phanz-national-awards-2020
Interesting to follow up your link. Baker has done some good stuff over the years. Somehow his constant commentary is being presented to undermine the managed isolation.
Genuinely not following that – is Baker's consistent advocacy/support for the managed isolation, testing and quarantining of those arriving in NZ being presented in a way that attempts to undermine our managed isolation programme? It's probably somewhere in the post and I've missed it – sorry.
The difference is that plan B are reactive not proactive,the mirror symmetry is different.
https://twitter.com/simonfrans/status/1338510819596890113/photo/1
https://twitter.com/yaneerbaryam/status/1338120658534842368
If this is the quality of the "research" then the Universities need to look seriously at their hiring practices. As well they need to develop some ethical standards around academics that rely on their Uni credentials when they are giving opinions way outside their lane where they have no specialist qualification whatsoever. My personal favourite was the lawyer trying to opine on the stats and maths underlying transmission!!!
‘As well they need to develop some ethical standards around academics that rely on their Uni credentials when they are giving opinions way outside their lane where they have no specialist qualification whatsoever’.
You mean media stars like Hendy (who is a physicist) or Wiles (who is a microbiologist)? Neither has published on epidemiology pre-Covid. Thornley in contrast has actually done epidemiological work pre-Covid (as of course, has Baker).
And Gorman (brain trauma specialist).
You strike me as a B & W kind of a person.
Hendy has been staying fairly close to his knitting, IMO. In his work, he develops and uses “either mathematical models or computer simulation methods, and frequently both”. https://unidirectory.auckland.ac.nz/profile/shaun-hendy
You’ll also note that Hendy has been awarded the Prime Minister's Science Media Communication Prize. Coincidentally, Wiles also is a recipient of the same Prize.
Unlike, Thornley, who has a fairly limited track record in epidemiology of infectious diseases, Hendy and Wiles are strong and experienced science communicators and this has been an important part of their jobs for a number of years and it shows. In other words, they are doing their jobs and they are doing it well, IMHO.
Praise Hendy all you want. But a model that had been constructed by or with epidemiologists would not have predicted 80000 deaths, a figure that we now know to be kind of absurd because of unrealistic assumptions underpinning the model. Also, a 'communication' award is a measure of the ability to communicate, not of professional expertise.
Please keep up if you want to contribute to an informed debate.
Hendy’s infamous paper from March 2020, in which they presented several model predictions, was based on work and a model by Baker and colleagues.
If you had followed this science story, you would know that they have moved on with the data & information since then. For example, here’s is their latest publication: https://www.tepunahamatatini.ac.nz/2020/12/16/modelling-support-for-the-continued-elimination-strategy/
OMG! Have you been living under a rock? And you have a subscription to Web of Science!?
https://www.wgtn.ac.nz/explore/study-areas/communication/study?subject=science-communication
https://www.wgtn.ac.nz/science/about/news/new-science-communication-major-in-2020
https://www.otago.ac.nz/science-communication/index.html
https://www.otago.ac.nz/courses/subjects/sccm.html
https://www.careers.govt.nz/qualifications/view/OO0462/7007#tab_key_information_for_students
The fact that they have moved on from their claim of 80000 does not in any way negate the fact that they made that claim in the first place. I doubt that anyone working within the boundaries of their expertise would so spectacularly err.
And the fact that most universities offer programs in communications (something that I am particularly familiar with btw) is actually entirely irrelevant to the point I was making, which is that the ability to communicate to the public well via the media, and scientific expertise and excellence, are absolutely not the same thing. They both propel progress but they are very, very different. And you think that I am the one living under a rock??!?
They did not err, as such. They took a model initially developed by Baker and co-workers, adapted it, and ran several simulations. In basic terms, these are what-if scenarios in which you vary the model input [parameters] and compare the different outcomes. As such, the numbers produced, i.e. outcomes, are not necessarily to be taken literally – they usually have probabilities associated with them, e.g. confidence interval, etc. – but in this case to inform and/or recommend public health measures and actions, which is why they provided it to the Government. The Government and MoH took these on board and the rest is history.
I’ll have to take your word for it, again, that you are familiar with programs in communications at universities but I cannot see it in your comments, I’m sorry to say. You made your point very poorly. Stop communicating like somebody from the stone age if you want to avoid the illusion that you have been living under a rock.
In any case, specialist scientific expertise and science communication often go hand-in-hand. Hendy wasn’t asked for and didn’t offer assistance or his professional views on vaccines, did he? He did what he is good at, i.e. specialises in, and he communicated this, which he also specialises in. Science communication is now becoming a specialism in its own right.
Wow. just wow. I always conclude when someone goes 'ad hominem' in their responses to me (as you keep doing) rather than sticking to the matter at hand, and keeps going off in tangents, that they are having quite some difficulty in articulating a convincing response. And while I don't begin to agree with your response and could keep responding ad infinitum, I don't actually think that keeping this going will achieve anything useful. So, I am actually going to leave the discussion at this point and the readers can read both our sets of comments and make of them what they will.
Oh, and feel free to have the last word using any ad-hominem words of your choice. Surely you can do better than 'stone age' and 'living under a rock''.
I'll have the last word.
That was not an ad-hominem from Incognito. You just chose to read it that way. As for the allegation Incog is going off on a tangent… that is also incorrect.
From my own background in science based forecasting techniques, Incognito's explanation is exactly how it works. You run a series of models based on possibilities then you eventually choose the model which ends up fitting the correct scenario as it starts to play out. In doing so, those who might be affected are afforded an opportunity to prepare in advance should the worst scenario eventuate.
And if you cannot see the value of such a mode of operation, then I have to conclude you really do not know what you are talking about.
BTW, dunno if anyone's linked to it recently. Here's the document journos extrapolated out to 80,000 dead.
Couple of points to note – firstly, 80k was the predicted result for zero response on the public health front.. Not even isolating cases or trying to get social distancing going. Cancelling elective zurgeries to bring up ICU capacity to 500 beds seems to be it, not in any way trying to lower cases. So worst response imaginable (maybe US federal level 🙁 ).
Second, even though the responses had a range of inputs, the disease in the model did not. They actually low-balled some of the numbers, but the issue here is that while they were reasonable estimates for NZ, Table 1 shows that things like hospitalisation rates can have quite wide confidence intervals. But the ICU admission rate they plugged into the model (1.25% infection) was about a quarter of the mid-range calculation (5.55%). But the actual range of ICU values in table1 is 3.29% — 7.82%. CFR is 0.90% –1.41% — 1.92%.
The goal was not to definitively state the number of NZers who would die. The goal was to establish a rough baseline and illustrate how different interventions would affect that outcome.
But that having been said, the projected pop fatality rate of 0.0004% if all controls were imposed isn't too far off (by my late night math) the 25 dead we have so far. So that end of the model seems accurate enough…
Yup, that sums it up very nicely in my view, thank you, and your “late night math” is pretty spot on 🙂
Hendy, Baker, and co-workers are doing some solid science and making it available to whomever wants to absorb it. They are setting a very high bar for Plan B, which is falling way short in the quality of their arguments and supporting evidence; they must lift their game or stop making noise.
Hendy, Baker, and co-workers have co-authored a recent paper, which has not yet been peer-reviewed): https://cpb-ap-se2.wpmucdn.com/blogs.auckland.ac.nz/dist/d/75/files/2020/11/Binny_et_al_Early_interventions_forTPMwebpage_9Nov.pdf.
Because it is highly topical to the discussion threads under this Post and highly instructive as to the methodology they are using I’ll highlight some bits from it, in order to edify further interested readers of The Standard.
In the Executive Summary, they summarise what they did:
They list the important results or output from their model simulations, which contain no surprises and mostly fairly self-explanatory:
This is probably their most important finding, from the model simulations, which basically states that Alert Level 4 had the greatest bearing on the key measures:
This is a pertinent sentence in their Introduction:
They come back to this in their Discussion, which highlights why direct comparisons between countries are difficult if not impossible. It also point to the fact that things change over time meaning that predictive models are almost never 100% accurate:
At least one of their key measures, i.e. the probability of elimination, influenced Government decisions:
First, they checked that their model was fit-for-purpose and gave an and gave an accurate representation of the actual and real numbers, which it does well:
Furthermore, (these) models need constant updating and refining:
Lastly, this may touch upon some of the concerns raised by weka and Rosemary McDonald although it is not very specific:
HTH
The fact that they have moved on from their claim of 80000 does not in any way negate the fact that they made that claim in the first place. I doubt that anyone working within the boundaries of their expertise would so spectacularly err.
Back in March there were many initial estimates floating around that the IFR pf COVID was well over 1%. At the time an estimate of 80,000 was well within the bounds of possibility … much higher even.
Hendy and Wiles are strong and experienced science communicators and this has been an important part of their jobs for a number of years and it shows. In other words, they are doing their jobs and they are doing it well, IMHO.
Hmmm…Wiles clearly (like many of us) found the whole pandemic/Lockdown thing a tad unsettling. This was evidenced by her seeming to forget that most of us have a enough intelligence and life experience to recognize and manage risk for ourselves. Just present the data and let us make our own minds up.The stupid animations became irritating after a remarkably short space of time…and usually I have a lot of respect for Morris's work.
Back in early March it was evident that she had not yet recognized that there were no experts on Te Virus and that in the interests of protecting those most vulnerable from these diseases it would be prudent, nay, morally required to take the precautionary approach and treat all like we were infected. https://thespinoff.co.nz/science/05-03-2020/can-you-catch-covid-19-from-someone-without-symptoms/
This divvery piece was followed by her mini thesis on the pros and cons of mask wearing…https://thespinoff.co.nz/society/06-04-2020/siouxsie-wiles-toby-morris-should-we-all-be-wearing-face-masks-to-prevent-covid-19-spread/ …which still held the 'wait for the evidence ' line before promoting mask wearing by health and disability workers.
Meanwhile… https://www.stuff.co.nz/national/health/coronavirus/120950545/coronavirus-waikato-hospital-doctor-says-compulsory-masks-vital-to-stopping-covid19 … but what would he know? In the early days she failed, like all our other frontline mouthpieces, to promote the precautionary approach…for this she (and the others) will never be forgiven. Vulnerable people were put at risk while they fucked around waiting for the "evidence".
Wiles is awesomely good at communicating whatever the official narrative might be at the time and on the day maybe if the wind is from the right quarter and it is the appropriate phase of the moon. The need for 'evidence' is strong in this one and her credibility took her further dive in our whanau when she popped out this particular instruction.
The general response to this was 'Ffs Wiles…make your fucking mind up!'
Remember back in the Dark Days of Key? When awards from the Top Floor heralded a plummet in professional credibility?
Yeah, 2m 'cos science says is really problematic when not qualified (choir singing, ffs). The science wouldn't have been *that sure, it would have been based on a specific set of criteria that may or may not be applicable to many situations. The whole 'we work with the science at the time and update as we go' is not the best approach on its own when dealing with complex systems like viral spread and human behaviour.
What irks me is the lack of awareness that organisations like the MoH are working on statistical probabilities across populations and that this means individuals can and do fall through the cracks.
I hear you but will all due respect, I think you have the wrong end of the stick in this case.
Please let me explain why I think that.
Wiles acted as a Science Communicator and made the fast-moving science accessible to many at a time when everybody was hungry for solid & sound information. She mostly managed to avoid dumbing down the science. As a scientist, she also avoided heavy speculation and long extrapolation of the available data & information. It was important, then more than ever, to avoid creating more uncertainty and confusion in the minds of the people by having to correct and/or retract statements about the science of Covid-19. So, yes, this meant cautious statements and a wait & see approach. Wiles had to and was operating within the boundaries of science, not short-cuts, no cutting corners, no reckons, et cetera.
AFAIK, Wiles was and is not a member of any Task Force or Advisory Group or the likes. She was a “mouthpiece” for [the] science. She was also not involved in setting policy, which is and was not her job or responsibility either. Moreover, she could not cover all science either. But she did a good job, by and large, and covered much and covered it well, IMHO. It was up to others to add, complement, correct, and/or provide counter arguments, as and when required, e.g. MoH officials and the PM. At the same time, she had to be careful not to undermine the official Government lines as this could have created confusion and have seeded doubts & distrust. I hazard a guess that even Siouxsie Wiles had to bite her tongue a few times 😉
Lastly, you say this:
That is neither here nor there. The Prime Minister's Science Communication Prize is not political like knighthoods, for example. The prize and process is managed by the Royal Society Te Apārangi and the winner is determined by an independent selection panel.
HTH
Point to one bit of evidence showing the new strain being more contagious. You want. Top doctors doubt the claim.
[Who are those “top doctors”? Do they exist only in your imagination?
Why don’t you provide names and links to three of those mythical “top doctors” so we can check that you’re not making up things. You will be in Pre-Moderation until you oblige or opt for a long vacation in the wop wops – Incognito]
[See you in one month – Incognito]
Public Health England reckons it has both epidemiological data and biological plausibility for the new variant having a reproductive advantage over previous variants. As of a week ago (which is a long time in politics and an eternity in this bloody pandemic, so who the fuck knows what the data says today).
See my Moderation note @ 1:40 AM.
There is one report done which hasn't been peer reviewed.
I am impressed!!
\sarc
you asked to be pointed to one bit of evidence. Job done.
Meh. When I first looked at the stats I thought I was reading it wrong – thinking it could not be possible for one strain to suddenly go from a single case to the dominant infection type so fast.
The earliest samples in which B.1.1.7 was reported were taken on 20 and 21 Sep in the UK, AFAIK. Based on its spread, models suggest that this new variant might be up to 70 percent more transmissible, which is consistent with some of its mutations in the spike protein and the fact that it and similar mutations have been found in other areas of the World.
See my second Moderation note @ 1:40 AM.
The key word is "academics" they got through med school and found that healing obese, semiliterate people and whining "worried well" was not suited to their "high achievement drive" so a chance of tenure and (notice the joint authorship) no direct, personal responsibility was irresistible. Bless the doctors who use their training to get on with the job and fuck the shitheads who authored this piece of mealy mouthed claptrap.