 The more difficult end to the vaccination programme
The more difficult end to the vaccination programme
Written By:
- Date published:
8:26 am, September 23rd, 2021 - 204 comments
Categories: covid-19, health, Judith Collins, trevor mallard -
Tags:
We are reaching an interesting stage in the vaccination program. The country’s recent vaccination roll out has been on steroids and we are now in a position where 80% of the target population should be vaccinated within the next month or so. We were slow starters, mainly because we were not subject to a pandemic that was killing our people and clogging our health systems, so we were able to have an orderly and properly organised roll out instead of panicking. But ever since the response has accelerated.
The complaints about the speed of the roll out have continued. But to be frank they miss the point. Our vaccination rate in comparison to the rest of the OECD is improving and our death rate is phenomenally good.
We are at the bottom of this graph, hidden because our ranking is so low.
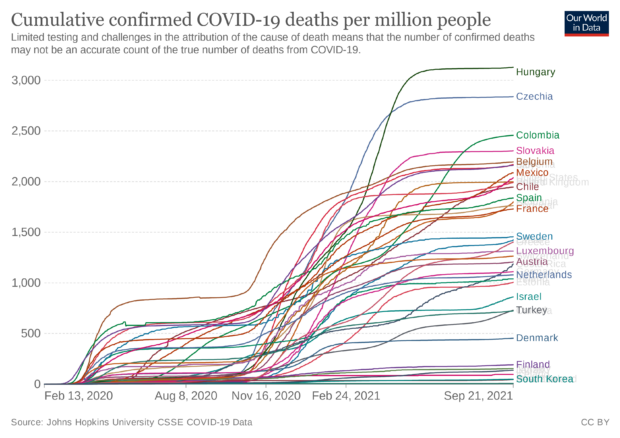
Our death rate, at 5.6 deaths per million people is at the bottom of the OECD ranking. The second best country is Australia at 46 deaths per million, followed by South Korea at 47 and Iceland at 96. If we had emulated Australia’s performance, second best in the OECD, there would have been 230 deaths, if we had performed as well as Denmark, an advanced nation with a superb health system the body count would have been 2,250. And if we had been as bad as Hungary there would have been over 15,000 deaths. Choose your preference.
Novelty campaigns such as the Shot Bro bus and the suggested KFC for jabs will have some effect particularly in poorer areas that are suffering the brunt of the latest infections. But we are now getting to the situation where we are reaching the reluctant and different techniques for this group will be required.
Throughout the world there are a variety of measures being used, from the coaxing and persuasion to the more gnarly use of regulatory might. Vaccine passports will soon be a reality. If you cannot prove you have been vaccinated then you may not be able to fly or attend concerts or even visit restaurants.
Employers will be under some pressure. How do you balance the right of a staff member to determine what health treatment they receive with the need to provide a safe workspace?
The more public facing the role the more likely that the right to refuse medical treatment is going to be overridden by policy decisions setting reasonable legal limits that can be demonstrably justified in a free and democratic society which is doing with a pandemic.
Trevor Mallard has sparked the debate by wondering if non vaccinated Parliamentary staffers should work from home and not at the Parliamentary precinct.
Handling of the end of the roll out will be critical. We are now moving from the highly motivated though the general population and into the reluctant sector of the population. And the virus does not discriminate. All it seeks is a warm body to propagate in.
This is why among all of her recent misdemeanors Judith Collins claiming that we should not make vaccination compulsory and that we will end up with two classes of people is so irresponsible. Publicly feeding into anti vaccination feelings is highly irresponsible. Although she is right in one respect. There will be two classes of people, vaccinated people for who a covid infection will on most occasions be no more than an irritant and unvaccinated people who will face the prospect of a lingering death.
Persuasion is still the most effective technique. If a family member, friend or work colleague is reluctant this information may help.
Otherwise there is always this Family Guy video.
https://www.youtube.com/watch?v=zDQuwkJIBaY
204 comments on “The more difficult end to the vaccination programme ”
- Comments are now closed
- Comments are now closed
CommentsOpinions
Recent Comments
FeedsPartyGovtMedia
- Donald Trump’s first three months: rude, raucous and rogue
 Sunday marks three months since Donald Trump’s inauguration as US president. What a ride: the style rude, language raucous, and the results rogue. Beyond manners, rudeness matters because tone signals intent as well as personality. ...2 hours ago
Sunday marks three months since Donald Trump’s inauguration as US president. What a ride: the style rude, language raucous, and the results rogue. Beyond manners, rudeness matters because tone signals intent as well as personality. ...2 hours ago - Taiwan: the sponge that soaks up Chinese power
Taiwan has an inadvertent, rarely acknowledged role in global affairs: it’s a kind of sponge, soaking up much of China’s political, military and diplomatic efforts. Taiwan soaks up Chinese power of persuasion and coercion that ...16 hours ago
- Women in combat roles strengthen our defence force
The Ukraine war has been called the bloodiest conflict since World War II. As of July 2024, 10,000 women were serving in frontline combat roles. Try telling them—from the safety of an Australian lounge room—they ...16 hours ago
- China targets Canada’s election—and may be targeting Australia’s
Following Canadian authorities’ discovery of a Chinese information operation targeting their country’s election, Australians, too, should beware such risks. In fact, there are already signs that Beijing is interfering in campaigning for the Australian election ...16 hours ago
- Climate Adam: Climate Scientist Reacts to Elon Musk
 This video includes personal musings and conclusions of the creator climate scientist Dr. Adam Levy. It is presented to our readers as an informed perspective. Please see video description for references (if any). From "founder" of Tesla and the OG rocket man with SpaceX, and rebranding twitter as X, Musk has ...17 hours ago
This video includes personal musings and conclusions of the creator climate scientist Dr. Adam Levy. It is presented to our readers as an informed perspective. Please see video description for references (if any). From "founder" of Tesla and the OG rocket man with SpaceX, and rebranding twitter as X, Musk has ...17 hours ago - Rattus Interneticus: Otago’s Internet Saga
 Back in February 2024, a rat infestation attracted a fair few headlines in the South Dunedin Countdown supermarket. Today, the rats struck again. They took out the Otago-Southland region’s internet connection. https://www.stuff.co.nz/nz-news/360656230/internet-outage-hits-otago-and-southland Strictly, it was just a coincidence – rats decided to gnaw through one fibre cable, while some hapless ...17 hours ago
Back in February 2024, a rat infestation attracted a fair few headlines in the South Dunedin Countdown supermarket. Today, the rats struck again. They took out the Otago-Southland region’s internet connection. https://www.stuff.co.nz/nz-news/360656230/internet-outage-hits-otago-and-southland Strictly, it was just a coincidence – rats decided to gnaw through one fibre cable, while some hapless ...17 hours ago - Spin (and obfuscation)
 I came in this morning after doing some chores and looked quickly at Twitter before unpacking the groceries. Someone was retweeting a Radio NZ story with the headline “Reserve Bank’s budget to be slashed by 25%”. Wow, I thought, the Minister of Finance has really delivered this time. And then ...19 hours ago
I came in this morning after doing some chores and looked quickly at Twitter before unpacking the groceries. Someone was retweeting a Radio NZ story with the headline “Reserve Bank’s budget to be slashed by 25%”. Wow, I thought, the Minister of Finance has really delivered this time. And then ...19 hours ago - Little’s pitch
 So, having teased it last week, Andrew Little has announced he will run for mayor of Wellington. On RNZ, he's saying its all about services - "fixing the pipes, making public transport cheaper, investing in parks, swimming pools and libraries, and developing more housing". Meanwhile, to the readers of the ...19 hours ago
So, having teased it last week, Andrew Little has announced he will run for mayor of Wellington. On RNZ, he's saying its all about services - "fixing the pipes, making public transport cheaper, investing in parks, swimming pools and libraries, and developing more housing". Meanwhile, to the readers of the ...19 hours ago - Our Rough Beast.
 And what rough beast, its hour come round at last,Slouches towards Bethlehem to be born?W.B. Yeats, The Second Coming, 1921ALL OVER THE WORLD, devout Christians will be reaching for their bibles, reading and re-reading Revelation 13:16-17. For the benefit of all you non-Christians out there, these are the verses describing ...19 hours ago
And what rough beast, its hour come round at last,Slouches towards Bethlehem to be born?W.B. Yeats, The Second Coming, 1921ALL OVER THE WORLD, devout Christians will be reaching for their bibles, reading and re-reading Revelation 13:16-17. For the benefit of all you non-Christians out there, these are the verses describing ...19 hours ago - What does India Want? What is New Zealand willing to give?
22 hours ago
- President Trump is redefining America’s international role, and Australia has influence
In the week of Australia’s 3 May election, ASPI will release Agenda for Change 2025: preparedness and resilience in an uncertain world, a report promoting public debate and understanding on issues of strategic importance to ...23 hours ago
- Simeon Brown Gaslights Doctors
 Yesterday, 5,500 senior doctors across Aotearoa New Zealand voted overwhelmingly to strike for a day.This is the first time in New Zealand ASMS members have taken strike action for 24 hours.They are asking the government to fund them and account for resource shortfalls.Vacancies are critical - 45-50% in some regions.The ...23 hours ago
Yesterday, 5,500 senior doctors across Aotearoa New Zealand voted overwhelmingly to strike for a day.This is the first time in New Zealand ASMS members have taken strike action for 24 hours.They are asking the government to fund them and account for resource shortfalls.Vacancies are critical - 45-50% in some regions.The ...23 hours ago - ACT’s “Tough on Crime” Facade Crumbles with Jago’s Appeal
 23 hours ago
23 hours ago - Judith Collins’ Hypocrisy: War Drums Over Welfare
Judith Collins is a seasoned master at political hypocrisy. As New Zealand’s Defence Minister, she's recently been banging the war drum, announcing a jaw-dropping $12 billion boost to the defence budget over the next four years, all while the coalition of chaos cries poor over housing, health, and education.Apparently, there’s ...1 day ago
- Making the most of it
 I’m on the London Overground watching what the phones people are holding are doing to their faces: The man-bun guy who could not be less impressed by what he's seeing but cannot stop reading; the woman who's impatient for a response; the one who’s frowning; the one who’s puzzled; the ...1 day ago
I’m on the London Overground watching what the phones people are holding are doing to their faces: The man-bun guy who could not be less impressed by what he's seeing but cannot stop reading; the woman who's impatient for a response; the one who’s frowning; the one who’s puzzled; the ...1 day ago - Maranga Ake
 You don't have no prescriptionYou don't have to take no pillsYou don't have no prescriptionAnd baby don't have to take no pillsIf you come to see meDoctor Brown will cure your ills.Songwriters: Waymon Glasco.Dr Luxon. Image: David and Grok.First, they came for the Bottom FeedersAnd I did not speak outBecause ...1 day ago
You don't have no prescriptionYou don't have to take no pillsYou don't have no prescriptionAnd baby don't have to take no pillsIf you come to see meDoctor Brown will cure your ills.Songwriters: Waymon Glasco.Dr Luxon. Image: David and Grok.First, they came for the Bottom FeedersAnd I did not speak outBecause ...1 day ago - Bernard’s Dawn Chorus & Pick ‘n’ Mix for Wednesday, April 16
 The Health Minister says the striking doctors already “well remunerated,” and are “walking away from” and “hurting” their patients. File photo: Lynn GrievesonLong stories short from our political economy on Wednesday, April 16:Simeon Brown has attacked1 doctors striking for more than a 1.5% pay rise as already “well remunerated,” even ...1 day ago
The Health Minister says the striking doctors already “well remunerated,” and are “walking away from” and “hurting” their patients. File photo: Lynn GrievesonLong stories short from our political economy on Wednesday, April 16:Simeon Brown has attacked1 doctors striking for more than a 1.5% pay rise as already “well remunerated,” even ...1 day ago - Strengthening Australia’s space cooperation with South Korea
The time is ripe for Australia and South Korea to strengthen cooperation in space, through embarking on joint projects and initiatives that offer practical outcomes for both countries. This is the finding of a new ...1 day ago
- They Can Only Talk About One Thing
 Hi,When Trump raised tariffs against China to 145%, he destined many small businesses to annihilation. The Daily podcast captured the mass chaos by zooming in and talking to one person, Beth Benike, a small-business owner who will likely lose her home very soon.She pointed out that no, she wasn’t surprised ...1 day ago
Hi,When Trump raised tariffs against China to 145%, he destined many small businesses to annihilation. The Daily podcast captured the mass chaos by zooming in and talking to one person, Beth Benike, a small-business owner who will likely lose her home very soon.She pointed out that no, she wasn’t surprised ...1 day ago - National’s Inflation Shame: Kiwis Pay the Price
National’s handling of inflation and the cost-of-living crisis is an utter shambles and a gutless betrayal of every Kiwi scraping by. The Coalition of Chaos Ministers strut around preaching about how effective their policies are, but really all they're doing is perpetuating a cruel and sick joke of undelivered promises, ...1 day ago
- Winston’s Mate Rhys Williams Has Been Unmasked
Most people wouldn't have heard of a little worm like Rhys Williams, a so-called businessman and former NZ First member, who has recently been unmasked as the venomous troll behind a relentless online campaign targeting Green Party MP Benjamin Doyle.According to reports, Williams has been slinging mud at Doyle under ...2 days ago
- Idiocy, Opportunity
 Illustration credit: Jonathan McHugh (New Statesman)The other day, a subscriber said they were unsubscribing because they needed “some good news”.I empathised. Don’t we all.I skimmed a NZME article about the impacts of tariffs this morning with analysis from Kiwibank’s Jarrod Kerr. Kerr, their Chief Economist, suggested another recession is the ...2 days ago
Illustration credit: Jonathan McHugh (New Statesman)The other day, a subscriber said they were unsubscribing because they needed “some good news”.I empathised. Don’t we all.I skimmed a NZME article about the impacts of tariffs this morning with analysis from Kiwibank’s Jarrod Kerr. Kerr, their Chief Economist, suggested another recession is the ...2 days ago - US allies must band together in weapons development
Let’s assume, as prudence demands we assume, that the United States will not at any predictable time go back to being its old, reliable self. This means its allies must be prepared indefinitely to lean ...2 days ago
- I’ve been reading
Over the last three rather tumultuous US trade policy weeks, I’ve read these four books. I started with Irwin (whose book had sat on my pile for years, consulted from time to time but not read) in a week of lots of flights and hanging around airports/hotels, and then one ...2 days ago
- This is not the time for increasing Indonesia’s defence spending
Indonesia could do without an increase in military spending that the Ministry of Defence is proposing. The country has more pressing issues, including public welfare and human rights. Moreover, the transparency and accountability to justify ...2 days ago
- FSU Supports Chris Milne’s Right to Make Death Threats
2 days ago
- Winston is inciting terrorism
That's the conclusion of a report into security risks against Green MP Benjamin Doyle, in the wake of Winston Peters' waging a homophobic hate-campaign against them: GRC’s report said a “hostility network” of politicians, commentators, conspiracy theorists, alternative media outlets and those opposed to the rainbow community had produced ...2 days ago
- Winston is inciting terrorism
That's the conclusion of a report into security risks against Green MP Benjamin Doyle, in the wake of Winston Peters' waging a homophobic hate-campaign against them: GRC’s report said a “hostility network” of politicians, commentators, conspiracy theorists, alternative media outlets and those opposed to the rainbow community had produced ...2 days ago
- Why has Hamish Campbell Gone Into Hiding?
National Party MP Hamish Campbell’s ties to the secretive Two By Twos "church" raises serious questions that are not being answered. This shadowy group, currently being investigated by the FBI for numerous cases of child abuse, hides behind a facade of faith while Campbell dodges scrutiny, claiming it’s a “private ...2 days ago
- Why has Hamish Campbell Gone Into Hiding?
National Party MP Hamish Campbell’s ties to the secretive Two By Twos "church" raises serious questions that are not being answered. This shadowy group, currently being investigated by the FBI for numerous cases of child abuse, hides behind a facade of faith while Campbell dodges scrutiny, claiming it’s a “private ...2 days ago
- The Government is cutting, just as the economic recovery is stalling
 The economy is not doing what it was supposed to when PM Christopher Luxon said in January it was ‘going for growth.’ Photo: Lynn Grieveson / The KākāLong stories short from our political economy on Tuesday, April 15:New Zealand’s economic recovery is stalling, according to business surveys, retail spending and ...2 days ago
The economy is not doing what it was supposed to when PM Christopher Luxon said in January it was ‘going for growth.’ Photo: Lynn Grieveson / The KākāLong stories short from our political economy on Tuesday, April 15:New Zealand’s economic recovery is stalling, according to business surveys, retail spending and ...2 days ago - For a safer Symonds Street
 This is a guest post by Lewis Creed, managing editor of the University of Auckland student publication Craccum, which is currently running a campaign for a safer Symonds Street in the wake of a horrific recent crash. The post has two parts: 1) Craccum’s original call for safety (6 ...2 days ago
This is a guest post by Lewis Creed, managing editor of the University of Auckland student publication Craccum, which is currently running a campaign for a safer Symonds Street in the wake of a horrific recent crash. The post has two parts: 1) Craccum’s original call for safety (6 ...2 days ago - Tuesday 15 April
 NZCTU President Richard Wagstaff has published an opinion piece which makes the case for a different approach to economic development, as proposed in the CTU’s Aotearoa Reimagined programme. The number of people studying to become teachers has jumped after several years of low enrolment. The coalition has directed Health New ...2 days ago
NZCTU President Richard Wagstaff has published an opinion piece which makes the case for a different approach to economic development, as proposed in the CTU’s Aotearoa Reimagined programme. The number of people studying to become teachers has jumped after several years of low enrolment. The coalition has directed Health New ...2 days ago - As China’s AI industry grows, Australia must support its own
The growth of China’s AI industry gives it great influence over emerging technologies. That creates security risks for countries using those technologies. So, Australia must foster its own domestic AI industry to protect its interests. ...2 days ago
- Luxon’s Economic Mismanagement
Unfortunately we have another National Party government in power at the moment, and as a consequence, another economic dumpster fire taking hold. Inflation’s hurting Kiwis, and instead of providing relief, National is fiddling while wallets burn.Prime Minister Chris Luxon's response is a tired remix of tax cuts for the rich ...2 days ago
- Girls and Boys
 Girls who are boys who like boys to be girlsWho do boys like they're girls, who do girls like they're boysAlways should be someone you really loveSongwriters: Damon Albarn / Graham Leslie Coxon / Alexander Rowntree David / Alexander James Steven.Last month, I wrote about the Birds and Bees being ...2 days ago
Girls who are boys who like boys to be girlsWho do boys like they're girls, who do girls like they're boysAlways should be someone you really loveSongwriters: Damon Albarn / Graham Leslie Coxon / Alexander Rowntree David / Alexander James Steven.Last month, I wrote about the Birds and Bees being ...2 days ago - Australia can learn from Britain on cyber governance
Australia needs to reevaluate its security priorities and establish a more dynamic regulatory framework for cybersecurity. To advance in this area, it can learn from Britain’s Cyber Security and Resilience Bill, which presents a compelling ...2 days ago
- Gordon Campbell On Why The US Stands To Lose The Tariff Wars
 Deputy PM Winston Peters likes nothing more than to portray himself as the only wise old head while everyone else is losing theirs. Yet this time, his “old master” routine isn’t working. What global trade is experiencing is more than the usual swings and roundabouts of market sentiment. President Donald ...2 days ago
Deputy PM Winston Peters likes nothing more than to portray himself as the only wise old head while everyone else is losing theirs. Yet this time, his “old master” routine isn’t working. What global trade is experiencing is more than the usual swings and roundabouts of market sentiment. President Donald ...2 days ago - Why is there no progress in Ukrainian war peace talks?
 President Trump’s hopes of ending the war in Ukraine seemed more driven by ego than realistic analysis. Professor Vladimir Brovkin’s latest video above highlights the internal conflicts within the USA, Russia, Europe, and Ukraine, which are currently hindering peace talks and clarity. Brovkin pointed out major contradictions within ...3 days ago
President Trump’s hopes of ending the war in Ukraine seemed more driven by ego than realistic analysis. Professor Vladimir Brovkin’s latest video above highlights the internal conflicts within the USA, Russia, Europe, and Ukraine, which are currently hindering peace talks and clarity. Brovkin pointed out major contradictions within ...3 days ago - Ani O’Brien has Zero Credibility
In the cesspool that is often New Zealand’s online political discourse, few figures wield their influence as destructively as Ani O’Brien. Masquerading as a champion of free speech and women’s rights, O’Brien’s campaigns are a masterclass in bad faith, built on a foundation of lies, selective outrage, and a knack ...3 days ago
- Australian policy does need more Asia—more Southeast Asia
The international challenge confronting Australia today is unparalleled, at least since the 1940s. It requires what the late Brendan Sargeant, a defence analyst, called strategic imagination. We need more than shrewd economic manoeuvring and a ...3 days ago
- EGU2025 – Picking and chosing sessions to attend on site in Vienna
This year's General Assembly of the European Geosciences Union (EGU) will take place as a fully hybrid conference in both Vienna and online from April 27 to May 2. This year, I'll join the event on site in Vienna for the full week and I've already picked several sessions I plan ...3 days ago
- Bookshelf: How China sees things
Here’s a book that looks not in at China but out from China. David Daokui Li’s China’s World View: Demystifying China to Prevent Global Conflict is a refreshing offering in that Li is very much ...3 days ago
- The Mirage of Chris Luxon’s Pre-Election Promises
The New Zealand National Party has long mastered the art of crafting messaging that resonates with a large number of desperate, often white middle-class, voters. From their 2023 campaign mantra of “getting our country back on track” to promises of economic revival, safer streets, and better education, their rhetoric paints ...3 days ago
- To counter anti-democratic propaganda, step up funding for ABC International
A global contest of ideas is underway, and democracy as an ideal is at stake. Democracies must respond by lifting support for public service media with an international footprint. With the recent decision by the ...3 days ago
- What was the story re Orr’s resignation?
It is almost six weeks since the shock announcement early on the afternoon of Wednesday 5 March that the Governor of the Reserve Bank, Adrian Orr, was resigning effective 31 March, and that in fact he had already left and an acting Governor was already in place. Orr had been ...3 days ago
- Monday 14 April
The PSA surveyed more than 900 of its members, with 55 percent of respondents saying AI is used at their place of work, despite most workers not being in trained in how to use the technology safely. Figures to be released on Thursday are expected to show inflation has risen ...3 days ago
- How to spot AI influence in Australia’s election campaign
Be on guard for AI-powered messaging and disinformation in the campaign for Australia’s 3 May election. And be aware that parties can use AI to sharpen their campaigning, zeroing in on issues that the technology ...3 days ago
- David Seymour – Arsehole of the Week
Strap yourselves in, folks, it’s time for another round of Arsehole of the Week, and this week’s golden derrière trophy goes to—drumroll, please—David Seymour, the ACT Party’s resident genius who thought, “You know what we need? A shiny new Treaty Principles Bill to "fix" all that pesky Māori-Crown partnership nonsense ...3 days ago
- Bernard’s Dawn Chorus and Pick ‘n’ Mix for Monday, April 14
 Apple Store, Shanghai. Trump wants all iPhones to be made in the USM but experts say that is impossible. Photo: Getty ImagesLong stories shortist from our political economy on Monday, April 14:Donald Trump’s exemption on tariffs on phones and computers is temporary, and he wants all iPhones made in the ...3 days ago
Apple Store, Shanghai. Trump wants all iPhones to be made in the USM but experts say that is impossible. Photo: Getty ImagesLong stories shortist from our political economy on Monday, April 14:Donald Trump’s exemption on tariffs on phones and computers is temporary, and he wants all iPhones made in the ...3 days ago - Unmasking the National Party’s Fascism
Kia ora, readers. It’s time to pull back the curtain on some uncomfortable truths about New Zealand’s political landscape. The National Party, often cloaked in the guise of "sensible centrism," has, at times, veered into territory that smells suspiciously like fascism. Now, before you roll your eyes and mutter about hyperbole, ...3 days ago
- Open Letter to Auckland Transport about Project K
This is a letter we will be sending to Auckland Transport to ask they return to the original consulted plans on the Karanga-a-Hape Station precinct integration project, after they released significant changes to designs last week. If you would like to be added as a signatory, please reach out to ...3 days ago
- The gas plan that’s sailing Australia into strategic peril
Australia’s east coast is facing a gas crisis, as the country exports most of the gas it produces. Although it’s a major producer, Australia faces a risk of domestic liquefied natural gas (LNG) supply shortfalls ...3 days ago
- Amateur Hour!
 Overnight, Donald J. Trump, America’s 47th President, and only the second President since 1893 to win non-consecutive terms, rolled back more of his “no exemptions, no negotiations” & “no big deal” tariffs.Smartphones, computers, and other electronics1 are now exempt from the 125% levies imposed on imports from China; they retain ...4 days ago
Overnight, Donald J. Trump, America’s 47th President, and only the second President since 1893 to win non-consecutive terms, rolled back more of his “no exemptions, no negotiations” & “no big deal” tariffs.Smartphones, computers, and other electronics1 are now exempt from the 125% levies imposed on imports from China; they retain ...4 days ago - 2025 SkS Weekly Climate Change & Global Warming News Roundup #15
A listing of 36 news and opinion articles we found interesting and shared on social media during the past week: Sun, April 6, 2025 thru Sat, April 12, 2025. This week's roundup is again published by category and sorted by number of articles included in each. The formatting is a ...4 days ago
- World Domination
 Just one year of loveIs better than a lifetime aloneOne sentimental moment in your armsIs like a shooting star right through my heartIt's always a rainy day without youI'm a prisoner of love inside youI'm falling apart all around you, yeahSongwriter: John Deacon.Morena folks, it feels like it’s been quite ...4 days ago
Just one year of loveIs better than a lifetime aloneOne sentimental moment in your armsIs like a shooting star right through my heartIt's always a rainy day without youI'm a prisoner of love inside youI'm falling apart all around you, yeahSongwriter: John Deacon.Morena folks, it feels like it’s been quite ...4 days ago - “I think I was, at that time, the only girl in Taranaki who ever wrote a line”
 “It's a history of colonial ruin, not a history of colonial progress,” says Michele Leggott, of the Harris family.We’re talking about Groundwork: The Art and Writing of Emily Cumming Harris, in which she and Catherine Field-Dodgson recall a near-forgotten and fascinating life, the female speck in the history of texts.Emily’s ...4 days ago
“It's a history of colonial ruin, not a history of colonial progress,” says Michele Leggott, of the Harris family.We’re talking about Groundwork: The Art and Writing of Emily Cumming Harris, in which she and Catherine Field-Dodgson recall a near-forgotten and fascinating life, the female speck in the history of texts.Emily’s ...4 days ago - Fact brief – Is the sun responsible for global warming?
Skeptical Science is partnering with Gigafact to produce fact briefs — bite-sized fact checks of trending claims. You can submit claims you think need checking via the tipline. Is the sun responsible for global warming? Greenhouse gas emissions from human activities, not solar variability, is responsible for the global warming observed ...4 days ago
- A Baptism in the Forest: Accepted
 Hitherto, 2025 has not been great in terms of luck on the short story front (or on the personal front. Several acquaintances have sadly passed away in the last few days). But I can report one story acceptance today. In fact, it’s quite the impressive acceptance, being my second ‘professional ...5 days ago
Hitherto, 2025 has not been great in terms of luck on the short story front (or on the personal front. Several acquaintances have sadly passed away in the last few days). But I can report one story acceptance today. In fact, it’s quite the impressive acceptance, being my second ‘professional ...5 days ago - Bernard’s Saturday Soliloquy for the week to April 12
 Six long stories short from our political economy in the week to Saturday, April 12:Donald Trump exploded a neutron bomb under 80 years of globalisation, but Nicola Willis said the Government would cut operational and capital spending even more to achieve a Budget surplus by 2027/28. That even tighter fiscal ...5 days ago
Six long stories short from our political economy in the week to Saturday, April 12:Donald Trump exploded a neutron bomb under 80 years of globalisation, but Nicola Willis said the Government would cut operational and capital spending even more to achieve a Budget surplus by 2027/28. That even tighter fiscal ...5 days ago - Budget 2025: delivering for whom?
 On 22 May, the coalition government will release its budget for 2025, which it says will focus on "boosting economic growth, improving social outcomes, controlling government spending, and investing in long-term infrastructure.” But who, really, is this budget designed to serve? What values and visions for Aotearoa New Zealand lie ...5 days ago
On 22 May, the coalition government will release its budget for 2025, which it says will focus on "boosting economic growth, improving social outcomes, controlling government spending, and investing in long-term infrastructure.” But who, really, is this budget designed to serve? What values and visions for Aotearoa New Zealand lie ...5 days ago - The Other Side
 Lovin' you has go to be (Take me to the other side)Like the devil and the deep blue sea (Take me to the other side)Forget about your foolish pride (Take me to the other side)Oh, take me to the other side (Take me to the other side)Songwriters: Steven Tyler, Jim ...5 days ago
Lovin' you has go to be (Take me to the other side)Like the devil and the deep blue sea (Take me to the other side)Forget about your foolish pride (Take me to the other side)Oh, take me to the other side (Take me to the other side)Songwriters: Steven Tyler, Jim ...5 days ago - It’s (past) time to get serious about funding Australia’s defence and security
In the week of Australia’s 3 May election, ASPI will release Agenda for Change 2025: preparedness and resilience in an uncertain world, a report promoting public debate and understanding on issues of strategic importance to ...5 days ago
- The Downward Spiral of Arise Church: Part 4
 Hi,Back in 2022 I spent a year reporting on New Zealand’s then-biggest megachurch, Arise, revealing the widespread abuse of hundreds of interns.That series led to a harrowing review (leaked by Webworm) and the resignation of its founders and leaders John and Gillian Cameron, who fled to Australia where they now ...5 days ago
Hi,Back in 2022 I spent a year reporting on New Zealand’s then-biggest megachurch, Arise, revealing the widespread abuse of hundreds of interns.That series led to a harrowing review (leaked by Webworm) and the resignation of its founders and leaders John and Gillian Cameron, who fled to Australia where they now ...5 days ago - Whatever the CCP says, regimes don’t have the rights of nations
All nation states have a right to defend themselves. But do regimes enjoy an equal right to self-defence? Is the security of a particular party-in-power a fundamental right of nations? The Chinese government is asking ...6 days ago
- Countervailing Trumpian Sense
 A modest attempt to analyse Donald Trump’s tariff policies.Alfred Marshall, whose text book was still in use 40 years after he died wrote ‘every short statement about economics is misleading with the possible exception of my present one.’ (The text book is 719 pages.) It’s a timely reminder that any ...6 days ago
A modest attempt to analyse Donald Trump’s tariff policies.Alfred Marshall, whose text book was still in use 40 years after he died wrote ‘every short statement about economics is misleading with the possible exception of my present one.’ (The text book is 719 pages.) It’s a timely reminder that any ...6 days ago - Uncertainty, Hierarchy and the Dilemma of Democracy.
 If nothing else, we have learned that the economic and geopolitical turmoil caused by the Trump tariff see-saw raises a fundamental issue of the human condition that extends beyond trade wars and “the markets.” That issue is uncertainty and its centrality to individual and collective life. It extends further into ...6 days ago
If nothing else, we have learned that the economic and geopolitical turmoil caused by the Trump tariff see-saw raises a fundamental issue of the human condition that extends beyond trade wars and “the markets.” That issue is uncertainty and its centrality to individual and collective life. It extends further into ...6 days ago - Strengthening South Korea’s national security by adopting the cloud
To improve its national security, South Korea must improve its ICT infrastructure. Knowing this, the government has begun to move towards cloud computing. The public and private sectors are now taking a holistic national-security approach ...6 days ago
- Workers’ Memorial Day 2025
28 April 2025 Mournfor theDead FightFor theLiving Every week in New Zealand 18 workers are killed as a consequence of work. Every 15 minutes, a worker suffers ...6 days ago
- Reset Pax Americana: the West needs a grand accord
The world is trying to make sense of the Trump tariffs. Is there a grand design and strategy, or is it all instinct and improvisation? But much more important is the question of what will ...6 days ago
- Poisoning The Well – It’s Not Just ACT
OPINION:Yesterday was a triumphant moment in Parliament House.The “divisive”, “disingenous”, “unfair”, “discriminatory” and “dishonest” Treaty Principles Bill, advanced by the right wing ACT Party, failed.Spectacularly.11 MP votes for (ACT).112 MP votes against (All Other Parties).As the wonderful Te Pāti Māori MP, Hana-Rāwhiti Maipi-Clarke said: We are not divided, but united.Green ...6 days ago
- The Pacific Response Group is making pleasing progress but needs more buy-in
The Pacific Response Group (PRG), a new disaster coordination organisation, has operated through its first high-risk weather season. But as representatives from each Pacific military leave Brisbane to return to their home countries for the ...6 days ago
- Friday 11 April
The Treaty Principles Bill has been defeated in Parliament with 112 votes in opposition and 11 in favour, but the debate about Te Tiriti and Māori rights looks set to stay high on the political agenda. Supermarket giant Woolworths has confirmed a new operating model that Workers First say will ...6 days ago
- A few wins, for now
 6 days ago
6 days ago - Aotearoa Wins!
 And this is what I'm gonna doI'm gonna put a call to you'Cause I feel good tonightAnd everything's gonna beRight-right-rightI'm gonna have a good time tonightRock and roll music gonna play all nightCome on, baby, it won't take longOnly take a minute just to sing my songSongwriters: Kirk Pengilly / ...6 days ago
And this is what I'm gonna doI'm gonna put a call to you'Cause I feel good tonightAnd everything's gonna beRight-right-rightI'm gonna have a good time tonightRock and roll music gonna play all nightCome on, baby, it won't take longOnly take a minute just to sing my songSongwriters: Kirk Pengilly / ...6 days ago
{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
- Release: Govt doesn’t know how to fund new hospitals
 The Government’s health infrastructure plan is big on promises but coy on where the money is coming from. ...19 hours ago
The Government’s health infrastructure plan is big on promises but coy on where the money is coming from. ...19 hours ago - Release: $10 million for only 215 students in charter schools
David Seymour is pouring $10 million into charter schools that only have 215 students enrolled. ...21 hours ago
- Release: Food prices further stretching the family budget
Families already stretched by rising costs will struggle with the news food prices are going up again. ...2 days ago
- Release: Mental health staff and patients at risk without plan
More people could be harmed if Minister for Mental Health Matt Doocey does not guarantee to protect patients and workers as the Police withdraw from supporting mental health call outs. ...3 days ago
- Release: Driver licensing proposal doesn’t put safety first
The Government’s proposal to change driver licensing rules is a mixed bag of sensible and careless. ...3 days ago
- Release: Students struggling as Govt sits on hands
The Government is continuing to sit on its hands as students struggle to pay rent due to delays with StudyLink. ...6 days ago
- Release: More must be done to stop children going hungry
More children are going hungry and statistics showing children in material hardship continue to get worse. ...6 days ago
- Greens continue to call for Pacific Visa Waiver
 The Green Party recognises the extension of visa allowances for our Pacific whānau as a step in the right direction but continues to call for a Pacific Visa Waiver. ...6 days ago
The Green Party recognises the extension of visa allowances for our Pacific whānau as a step in the right direction but continues to call for a Pacific Visa Waiver. ...6 days ago - More children going hungry under Coalition govt
The Government yesterday released its annual child poverty statistics, and by its own admission, more tamariki across Aotearoa are now living in material hardship. ...6 days ago
- Release: Longer wait for treatment under National
New Zealanders have waited longer to get an appointment with a specialist and to get elective surgery under the National Government. ...6 days ago
- Ka mate te Pire- Ka ora te mana o Te Tiriti o Waitangi me te iwi Māori
Today, Te Pāti Māori join the motu in celebration as the Treaty Principles Bill is voted down at its second reading. “From the beginning, this Bill was never welcome in this House,” said Te Pāti Māori Co-Leader, Rawiri Waititi. “Our response to the first reading was one of protest: protesting ...7 days ago
- Chris Hipkins speech: Treaty Principles Bill second reading
Normally, when I rise in this House to speak on a bill, I say it's a great privilege to speak on the bill. That is not the case today. ...7 days ago
- Release: End to the Treaty Principles Bill, but challenges remain ahead for Aotearoa
Ka mate te pire I te rā neiThe bill dies today ...7 days ago
- Ka mate te Pire, ka ora Te Tiriti o Waitangi – Treaty Principles Bill dead, Te Tiriti o Waitangi m...
The Green Party is proud to have voted down the Coalition Government’s Treaty Principles Bill, an archaic piece of legislation that sought to attack the nation’s founding agreement. ...7 days ago
- Member’s Bill an opportunity for climate action
A Member’s Bill in the name of Green Party MP Julie Anne Genter which aims to stop coal mining, the Crown Minerals (Prohibition of Mining) Amendment Bill, has been pulled from Parliament’s ‘biscuit tin’ today. ...7 days ago
- Release: Bill to make trading laws fairer passes first hurdle
Labour MP Kieran McAnulty’s Members Bill to make the law simpler and fairer for businesses operating on Easter, Anzac and Christmas Days has passed its first reading after a conscience vote in Parliament. ...7 days ago
- Release: Reserve Bank acts while Govt shrugs
Nicola Willis continues to sit on her hands amid a global economic crisis, leaving the Reserve Bank to act for New Zealanders who are worried about their jobs, mortgages, and KiwiSaver. ...1 week ago
- Release: Property Law Amendment Bill pulled from ballot
A Bill to protect first home buyers and others from bad faith property vendors has been drawn from the Member’s Ballot. ...1 week ago
- Release: More children at risk of losing family connections
Karen Chhour is proposing to scrap Oranga Tamariki targets which aim to connect more children under state care with family and their culture. ...1 week ago
- Release: David Parker made a difference – Hipkins
The Labour Leader today acknowledged and celebrated David Parker’s 23-year contribution to the Labour Party and to Parliament. ...1 week ago
- Release: David Parker to step down from Parliament
Long-serving Labour MP and former Minister David Parker has today announced his intention to leave Parliament. ...1 week ago
- Release: Flaws in Govt’s climate strategy will cost us money
The Government’s plan to achieve our climate goals falls short, and will cost New Zealanders money and jobs. ...1 week ago
- Green Party differing view on the Treaty Principles Bill
Read the Green Party's differing view on the Treaty Principles Bill, prepared by Tamatha Paul. ...1 week ago
- Te Pāti Māori Urges Governor-General to Block Repeal of 7AA
Today, the Oranga Tamariki (Repeal of Section 7AA) Amendment Bill has passed its third and final reading, but there is one more stage before it becomes law. The Governor-General must give their ‘Royal assent’ for any bill to become legally enforceable. This means that, even if a bill gets voted ...2 weeks ago
- Release: Abortion care quietly shelved amid staff shortage
Abortion care at Whakatāne Hospital has been quietly shelved, with patients told they will likely have to travel more than an hour to Tauranga to get the treatment they need. ...2 weeks ago
- Release: Govt guts Kāinga Ora, third of workforce under axe
The gutting of Kāinga Ora shows public housing is not a priority for this Government as it removes a third of the roles at the housing agency. ...2 weeks ago
- Release: Thousands of submissions excluded from Treaty Principles Bill report
Thousands of New Zealanders’ submissions are missing from the official parliamentary record because the National-dominated Justice Select Committee has rushed work on the Treaty Principles Bill. ...2 weeks ago
- Release: Uncertainty remains over the impact of tariffs
Today’s announcement of 10 percent tariffs for New Zealand goods entering the United States is disappointing for exporters and consumers alike, with the long-lasting impact on prices and inflation still unknown. ...2 weeks ago
- Release: Worst February for building consents in over a decade
The National Government’s choices have contributed to a slow-down in the building sector, as thousands of people have lost their jobs in construction. ...2 weeks ago
- Release: Labour supports Willie Apiata’s selfless act
Willie Apiata’s decision to hand over his Victoria Cross to the Minister for Veterans is a powerful and selfless act, made on behalf of all those who have served our country. ...2 weeks ago
- Te Pāti Māori MPs Denied Fundamental Rights in Privileges Committee Hearing
The Privileges Committee has denied fundamental rights to Debbie Ngarewa-Packer, Rawiri Waititi and Hana-Rawhiti Maipi-Clarke, breaching their own standing orders, breaching principles of natural justice, and highlighting systemic prejudice and discrimination within our parliamentary processes. The three MPs were summoned to the privileges committee following their performance of a haka ...2 weeks ago
- Release: Govt health and safety changes put workers at risk
Changes to New Zealand’s health and safety laws will strip back key protections for small businesses and put working Kiwis at greater risk. ...2 weeks ago
- Release: Kiwis worse off this April thanks to Govt choices
April 1 used to be a day when workers could count on a pay rise with stronger support for those doing it tough, but that’s not the case under this Government. ...2 weeks ago
- Release: Three more years for Interislander ferries
Winston Peters is shopping for smaller ferries after Nicola Willis torpedoed the original deal, which would have delivered new rail enabled ferries next year. ...2 weeks ago
- Release: Myanmar junta must stop the airstrikes
The Government should work with other countries to press the Myanmar military regime to stop its bombing campaign especially while the country recovers from the devastating earthquake. ...2 weeks ago
- Release: National failing to deliver on supermarkets
National is paying lip service to its promises to bring down the cost of living, failing to make any meaningful change in the grocery sector. ...2 weeks ago
No feed items found.
- Help Me Hera: How do I come out as a ‘Disney Millennial’?
 I’m sick of feeling ashamed of something that brings me so much joy. Want Hera’s help? Email your problem to helpme@thespinoff.co.nz Dear Hera, When I think of my childhood, I think of Disney. One of my earliest memories was getting dressed up as Snow White and prancing around for my ...52 minutes ago
I’m sick of feeling ashamed of something that brings me so much joy. Want Hera’s help? Email your problem to helpme@thespinoff.co.nz Dear Hera, When I think of my childhood, I think of Disney. One of my earliest memories was getting dressed up as Snow White and prancing around for my ...52 minutes ago - ‘They are like my children’: research reveals 4 types of indoor plant owners. Which one are you?
 Source: The Conversation (Au and NZ) – By Brianna Le Busque, Lecturer in Environmental Science, University of South Australia maramorosz/Shutterstock Walk into any home or workplace today, and you’re likely to find an array of indoor plants. The global market for indoor plants is growing fast – projected to ...1 hour ago
Source: The Conversation (Au and NZ) – By Brianna Le Busque, Lecturer in Environmental Science, University of South Australia maramorosz/Shutterstock Walk into any home or workplace today, and you’re likely to find an array of indoor plants. The global market for indoor plants is growing fast – projected to ...1 hour ago - Finance Minister Nicola Willis tells Reserve Bank to ‘show some restraint’ as budget sla...
 The budget has been slashed by about 25 percent. ...1 hour ago
The budget has been slashed by about 25 percent. ...1 hour ago - Cracks in social cohesion – the major parties must commit to reinvigorating multiculturalism
Source: The Conversation (Au and NZ) – By Andrew Jakubowicz, Emeritus Professor of Sociology, University of Technology Sydney In the run up to the May 3 election, questions are being raised about the value of multiculturalism as a public policy in Australia. They’ve been prompted by community tensions arising from ...2 hours ago
- State of the states: six experts on how the campaign is playing out around Australia
Source: The Conversation (Au and NZ) – By David Clune, Honorary Associate, Government and International Relations, University of Sydney The federal election campaign has passed the halfway mark, with politicians zig-zagging across the country to spruik their policies and achievements. Where politicians choose to visit (and not visit) give us ...2 hours ago
- People are ‘microdosing’ weight-loss drugs. A GP explains what to watch out for
Source: The Conversation (Au and NZ) – By Natasha Yates, General Practitioner, PhD Candidate, Bond University MillaF/Shutterstock Injectable medications originally developed for the treatment of diabetes are also effective for weight loss, and have surged in popularity for this purpose around the world. In Australia, Ozempic is approved for ...2 hours ago
- With the end of Flybuys NZ, what happens to the personal data of nearly 3 million Kiwis?
Source: The Conversation (Au and NZ) – By Lisa M. Katerina Asher, Doctoral Candidate, Business School, University of Sydney JuSun/Getty Images After almost three decades in New Zealand, loyalty programme Flybuys announced it would be closing in 2024. The company behind the scheme, Loyalty New Zealand, has since entered ...2 hours ago
- New Aussie film The Correspondent is an extraordinary retelling of Peter Greste’s story
Source: The Conversation (Au and NZ) – By Andrea Jean Baker, Senior Lecturer in Journalism, Monash University Maslow Entertainment The Correspondent is a film every journalist should see. There are no spoiler alerts. It is based on the globally-publicised jailing in Cairo in 2013 of Australian journalist Peter ...2 hours ago
- Health NZ report admits poor management of hospital facilities
A Health NZ report says it "cannot effectively plan for asset renewals, replacements or optimise maintenance strategies". ...3 hours ago
- Hospitals to be rebuilt in four stages under new $20b plan
Hospitals nationwide are set for upgrades – though at a more sedate pace than some might have hoped, writes Catherine McGregor in today’s extract from The Bulletin. To receive The Bulletin in full each weekday, sign up here. A blueprint for rebuilding After years of warnings and stocktakes, the government has ...3 hours ago
- NZ First donor launches airline war on Chatham Islands
 Visiting government and business leaders, disembarking an Air Force Hercules, were met this week by the unexpected sight of a big fresh-painted Boeing 737 freighter unloading at Chatham Island’s tiny airport.The growing trans-Tasman freight firm Texel Air took delivery of the 737-800 jet last month, taking its fleet to six ...3 hours ago
Visiting government and business leaders, disembarking an Air Force Hercules, were met this week by the unexpected sight of a big fresh-painted Boeing 737 freighter unloading at Chatham Island’s tiny airport.The growing trans-Tasman freight firm Texel Air took delivery of the 737-800 jet last month, taking its fleet to six ...3 hours ago - Defunding the police is good policy, actually
Suggestions of defunding the police have sparked uproar but it’s a sensible and noble goal, argue two crime researchers. When we both first saw the “attack” ads put up by some combination of the Sensible Sentencing Trust and the Campaign Company, we couldn’t fully grasp the framing of an “attack” ...5 hours ago
- The Beehive is lauding a big drop in violent crime. But what do the stats really say?
This week, a dramatic dip in the number of victims of violent crime was revealed, a remarkable turnaround in just eight months that the government was quick to take credit for. But, as Alice Neville explains, crime data is far from clear-cut. In September last year, the government announced a ...5 hours ago
- Daily crossword, Thursday 17 April
The post Daily crossword, Thursday 17 April appeared first on Newsroom. ...5 hours ago
- Act left out of loop on PM’s tariff alliance plans
As Christopher Luxon disputes claims of tariff plan disagreement, another coalition partner says it was in the dark The post Act left out of loop on PM’s tariff alliance plans appeared first on Newsroom. ...5 hours ago
- Newsroom daily quiz, Thursday 17 April
Loading…(function(i,s,o,g,r,a,m){var ql=document.querySelectorAll('A[data-quiz],DIV[data-quiz]'); if(ql){if(ql.length){for(var k=0;k<ql.length;k++){ql[k].id='quiz-embed-'+k;ql[k].href="javascript:var i=document.getElementById('quiz-embed-"+k+"');try{qz.startQuiz(i)}catch(e){i.start=1;i.style.cursor='wait';i.style.opacity='0.5'};void(0);"}}};i['QP']=r;i[r]=i[r]||function(){(i[r].q=i[r].q||[]).push(arguments)},i[r].l=1*new Date();a=s.createElement(o),m=s.getElementsByTagName(o)[0];a.async=1;a.src=g;m.parentNode.insertBefore(a,m)})(window,document,'script','https://take.quiz-maker.com/3012/CDN/quiz-embed-v1.js','qp');Got a good quiz question? Send Newsroom your questions.Keep playing
Newsroom daily quiz, Thursday 17 April 5 hours ago - Faith, hope and chocolate eggs
Chocolate eggs. Debates over shop opening hours. Traffic congestion as Kiwis take advantage of four days off in a row. Often it’s the last of the summer weather, or the first of the winter blast.This is the Easter break in New Zealand that most people recognise.But it’s not the same ...5 hours ago
- Get ready for even more Shein and Temu ads as Trump tariffs bite
Hefty charges will apply to cheap packages heading into the US from China from May 2, disrupting some of the world’s largest retailers The post Get ready for even more Shein and Temu ads as Trump tariffs bite appeared first on Newsroom. ...5 hours ago
- Peters’ desperation is PM’s gain
Comment: Treaty Principles Bill defeat and global campaign against Trump’s tariffs have given PM chance to assert himself over coalition The post Peters’ desperation is PM’s gain appeared first on Newsroom. ...5 hours ago
- Act’s ‘happy Māori’ AI image sparks internal change
An Act Party ad celebrating household savings under its Government used an AI-generated image titled ‘Happy Maori couple sits comfortably in a cozy living light room, generated ai’.There is nothing to stop a party from using an artificial image without disclosing it, per the Electoral Commission, and this is not ...5 hours ago
- Seymour seeks to spark a new ‘culture war’
After months of dealing with protesters in their masses, David Seymour is almost disappointed when his critics don’t show up in sufficient volume.Speaking at a lunchtime event, the Act Party leader says there has been “at least a 95 percent reduction in Gaza protesters since the last time I spoke ...5 hours ago
- Book of the Week: Naomi walks the earth
Down at the local hall a 50-strong community meeting had just finished and the crowd was milling around, catching up, pouring itself a last glass of wine, before home to bed. Two women came up to me wanting a conversation about Te Araroa, and I mentioned I’d just then finished ...5 hours ago
- Fiji defence minister draws flak for six-week trip to meet peacekeepers
RNZ Pacific Fiji’s Minister for Defence and Veteran Affairs is facing a backlash after announcing that he was undertaking a multi-country, six-week “official travel overseas” to visit Fijian peacekeepers in the Middle East. Pio Tikoduadua’s supporters say he should “disregard critics” for his commitment to Fijian peacekeepers, which “highlights a ...8 hours ago
- Election Diary: there were a couple of ‘moments’ in second Albanese-Dutton encounter
Source: The Conversation (Au and NZ) – By Michelle Grattan, Professorial Fellow, University of Canberra Two “moments” stuck out in Wednesday’s leaders’ debate, the second head-to-head of the campaign. Peter Dutton cut his losses over his faux pas this week when he wrongly named Indonesian president Prabowo Subianto as having ...9 hours ago
- Second leaders’ debate is a tame affair befitting a ‘deeply uninspiring’ campaign
Source: The Conversation (Au and NZ) – By Andy Marks, Vice-President, Public Affairs and Partnerships, Western Sydney University Prime Minister Anthony Albanese and Opposition Leader Peter Dutton have had their second showdown of the 2025 federal election campaign. The debate, hosted by the ABC, was moderated by David Speers in ...9 hours ago
- Poll shows Australians hate Trump policies and have lost trust in US, but still strongly believe in ...
Source: The Conversation (Au and NZ) – By Michelle Grattan, Professorial Fellow, University of Canberra Australians strongly disagree with key policies of US President Donald Trump, and have overwhelmingly lost trust in the United States to act responsibly in the world, according to the Lowy Institute’s 2025 poll. Despite ...10 hours ago
- NZ’s Palestine Forum calls on Luxon to take ‘firm stand’ over Israeli atrocities with temporar...
Asia Pacific Report A Palestinian advocacy group has called on NZ Prime Minister Christopher Luxon and Foreign Minister Winston Peters to take a firm stand for international law and human rights by following the Maldives with a ban on visiting Israelis. Maher Nazzal, chair of the Palestine Forum of New ...13 hours ago
- Bipartisanship On The Field And In The House
 MPs from across the political spectrum reveal they're a surprisingly collegial bunch. ...13 hours ago
MPs from across the political spectrum reveal they're a surprisingly collegial bunch. ...13 hours ago - Global Push Back Against Gender Equality A Growing Crisis In Aotearoa
Barriers to gender equality exist in many forms and in New Zealand, these barriers are worse for Māori, Pasifika, Asian, migrant, refugee, disabled, LGBTQIA+ and rural women, and Government action is required. ...17 hours ago
- We compared the Labor and Coalition’s income tax proposals to see who benefits most
Source: The Conversation (Au and NZ) – By John Hawkins, Senior Lecturer, Canberra School of Politics, Economics and Society, University of Canberra Shutterstock We now have the competing bids for our votes by the alternative governments on income tax policy. From Labor, future cuts to the lowest marginal ...17 hours ago
- Half of Australian landlords sell their investments after 2 years, adding to renters’ insecurity
Source: The Conversation (Au and NZ) – By Ranjodh B. Singh, Senior Economics and Finance Lecturer, Curtin University Marc Bruxelle/Shutterstock Australia’s renters have to battle rising rents and a lack of available properties. They also face ongoing instability. Our new research suggests half of all landlords sell their investment ...18 hours ago
- Labor and the Greens likely to gain Senate seats at the election
Source: The Conversation (Au and NZ) – By Adrian Beaumont, Election Analyst (Psephologist) at The Conversation; and Honorary Associate, School of Mathematics and Statistics, The University of Melbourne As well as the election for the full House of Representatives, there will be an election on May 3 for 40 of ...18 hours ago
- 3 in 4 meth users relapse – outcomes could improve if treatments considered the drug’s effect on...
Source: The Conversation (Au and NZ) – By Rebecca Bodeker, Teaching Assistant in Behavioural Psychology, University of Canterbury Getty Images Methamphetamine is New Zealand’s most harmful illicit drug and wastewater testing shows its use and availability are on the rise. Much of the harm results from reckless and ...19 hours ago
- This election, disinformation is swirling on Chinese social media. Here’s how it spreads
Source: The Conversation (Au and NZ) – By Fan Yang, Research fellow at Melbourne Law School, the University of Melbourne and the ARC Centre of Excellence for Automated Decision-Making and Society., The University of Melbourne Shutterstock/The Conversation Since 2024, the RECapture research team has been monitoring political disinformation and ...19 hours ago
- Politics with Michelle Grattan: Warwick McKibbin on trying to model economic certainty in uncertain ...
Source: The Conversation (Au and NZ) – By Michelle Grattan, Professorial Fellow, University of Canberra Global markets have remained on edge after Donald Trump’s “Liberation Day” tariffs caused panic worldwide. Now, more than ever, markets and economists are looking for trying to read the implications. Joining us from ...19 hours ago
- ER Report: A Roundup of Significant Articles on EveningReport.nz for April 16, 2025
ER Report: Here is a summary of significant articles published on EveningReport.nz on April 16, 2025. Trump’s racist, corrupt agenda – like a bank robbery in broad daylightEDITORIAL: By Giff Johnson, editor of the Marshall Islands Journal US President Donald Trump and his team is pursuing a white man’s racist ...19 hours ago
- Madness To Slash Reserve Bank Budget At A Time Of Economic Challenge
The bank’s inflation mandate is a key tool for economic management. It fights inflation so the economy can flourish without the damaging impacts of runaway inflation. ...19 hours ago
- There’s a new best hot cross bun in Auckland
Breaking news for those who just want a really good, classic hot cross bun. “This is the best hot cross bun I’ve ever had.” “I don’t usually like hot cross buns but fuck that was good.” Just two of the many overhead comments in The Spinoff office this morning after ...19 hours ago
- Trump’s racist, corrupt agenda – like a bank robbery in broad daylight
EDITORIAL: By Giff Johnson, editor of the Marshall Islands Journal US President Donald Trump and his team is pursuing a white man’s racist agenda that is corrupt at its core. Trump’s advisor Elon Musk, who often seems to be the actual president, is handing his companies multiple contracts as his ...20 hours ago
- Why the Coalition’s tone-deaf diss track was bound to hit all the wrong notes
Source: The Conversation (Au and NZ) – By Andy Ward, Senior Lecturer in Music, School of Business and Creative Industries, University of the Sunshine Coast Hip-hop is a cultural powerhouse that has infiltrated every facet of popular culture, across a global market. That said, one place you usually don’t see ...20 hours ago
Yes because coercion and suspension of civil liberties in a democracy is always a winning formula when strong arming people into taking experimental vaccines with indemnity for the manufacturer.
Just look at Melbourne. It all going swimmingly, right?
I have attempted to present both arguments neutrally and to highlight that this is not a simple issue and there is no simple answer.
Yes I do appreciate that you've been reasonably even-handed in this post. It does ask good questions.
Sadly I'm beginning to suspect they will have no good answers.
To jab, or not to jab, that is the question.
A good question, and a good answer was provided in an easy to understand graph posted by Macro on 14 Sept.
The current COVID-19 vaccines and treatments aren’t silver/magic bullets (not that any rational person would make such a claim), but imho they’re useful alternatives to the let 'er rip ‘solution’ that some are advocating. Time will tell.
But it is not (just) a (academic) question, it is a choice, or is it?
A choice for most Kiwis, imho, and an easy choice for me.
This epidemic, which isn't yet (and hopefully won’t become) the deadliest in NZ in my lifetime, poses a serious public health risk if global ‘COVID numbers’ are to be believed. Most Kiwi's have made good choices so far – let's keep calm and carry on vaccinating, washing hands, wearing masks, staying home and getting tested when sick, scanning/signing in, etc. etc., and "see what happens".
https://coronavirus.medium.com/white-house-finally-announces-coronavirus-plan-let-er-rip-326cb8b1342c
Choices have consequences.
If someone exercises the choice not to take a safe, free effective precaution against being a disease spreader, a reasonable consequence would be that nobody allows them on their premises as an employee or customer, because of their health and safety obligations.
The choice is preserved, the consequences of that choice are reasonable and proportionate..
All part of the choice, isn’t it? Or do you prefer a Clayton’s choice?
See also this: https://thestandard.org.nz/open-mike-23-09-2021/#comment-1818036.
For myself I'd say only if you choose to do so. If not then that's your right and should be respected.
I would prefer to wait and be sure its fully tested and any indemnity removed.
What do you even mean by "fully tested"? Pfizer went through the same tests as every other jab or drug does these days.
If you want to refuse a fully tested and approved treatment that's already been taken by hundreds of millions of people with an astonishingly good safety record and astonishingly high real world effectiveness, yes, you do have the right. But you don't have the right to be a willful health and safety risk to everyone else that gets near you.
So I'd prefer a medical officer then exercises their power under section 70 of the Health Act to keep you quarantined. At least until the government formalises vaccine passports and legislates to make it clear 'no jab, no job" policies are totally acceptable, even necessary, for employers to meet their health and safety obligations.
From your post:
Collins, in my view, is being completely disingenuous with this claim. Just the she-dog barking at EVERY car going past – again. From observing her as a Minister over several years, I would put money on it that – God forbid, were she the PM – she would be the PM most likely to make vaccinations compulsory.
Always likes to project herself as a strong authoritarian character.
And debate is worthwhile so I hope you don't take this as a personal rebuttal. My concern is that vaccines typically take 5 or more years to develop. I have taken them all my life so I'm someone who hates vaccines and scorns them.
I worry as many do I'm sure about the potential side effects and those that may arise in future? I also question why other well established medications are not being considered?
And as I say when does coercion by governments ever work well? Its not working well in France, its not working well in the UK and as for Australia as we seeing its not going so well.
I would say too we live in a democracy, people have rights and it worries me if they are not acknowledged now, will they be in the future?
I could say a lot more but these points will suffice for this discussion.
Thank you.
Potential side effects of vaccine: Feel tired, get a headache
Potential side effect of Covid-19: 1-2% chance of death, much higher chance of "long covid", permanent damage to lungs, brain or other organs.
"Status Quo Bias": a pattern of thinking where the risk of doing nothing is ignored, and the risk of doing something is exaggerated.
Yep. I got a slightly sore/tender upper arm at the injection site the next day, & woke up with a headache the morning after, after both jabs.
The injection itself was painless. I only knew it’d been done when the nurse said “All done!” And 2 ibuprofen at breakfast cured the headache completely in about 30 mins max.
Even the tender upper arm was gone within another 24 hours – and it didn’t stop me using that arm. It was a breeze.
I actually got hit kinda hard by the first one. About as bad as when I got Hep A, Hep B, polio booster, and rabies all in one session.
Arm was sore for three days, and the day after I felt really lethargic and just super-cold all over. It's the only day I've wanted a heater all winter, and the heater didn't help much.
If the second one hits harder like it does for most people, it'll be no fun at all. Kinda like only one day of a very mild flu.
Dream On. What do you think the "side effects" of NOT being vaccinated will be?
The health treatment in a safe work place conundrum is compounded by those more accident prone jobs which put workmates in a seriously compromised position in needing to give immediate cares to an injured non- vaccinated coworker.
Sugar gest more honey than vinegar. Less Bounties and more Bounty Bars. The imagination of the patrician state run can wild with a running menu from toughest 20% down to toughest .5%:
– Free KFC, or McDonalds, or Fish and Chips, for whole family
– Free haircuts. Great after lockdown
– Get your bond back if your household gets it
– $500 cash if you bring 5 unvaccinated people
– Free bicycle per person
– Free dog biscuits for a year
– Free kitten!
Will that kitten have had its shots?
The chip is inserted with the shot.
I wonder how the "5G tracking-chip" crowd explain the Government's insistence on the second jab?
The second shot is the Logan's Run pill with a secret timer for global population control.
… and what will be in the subsequent necessary booster shots!
Just keep Jabbing and anything is possible
Though well intended, this shows how far we amateurs are behind MoH experts, who, following evidence based science, are already rolling out bacon butties up and down the country.
That Taranaki initiative is excellent in a low-vaccination-rate DHB.
Free venison burgers for Southland, Fiordland, Westland and McKenzie Country.
I agree with Le Gros. Anti-vaxxers should not be allowed air-time and more needs to be done to prevent them from undermining the efforts to overcome this virus:
https://www.nzherald.co.nz/nz/covid-19-delta-outbreak-govt-concedes-big-mountain-to-climb-to-lift-vaccination-rate/E4KNJBYJYBANWL7EOWZLWN2Y4I/
I know an anti-vaxxer and they are not capable of rational thought, so trying to make them see sense does not work. You only have to look across the Tasman to see the aggressive antics they deploy and the danger they pose to everyone including the police. The ‘vaccine hesitant’ are a different story. Many of them are only hesitant because an anti-vaxxer has got to them.
I would go so far as making the distribution of anti-vax pamphlets a criminal offence. You have to fight fire with fire and this is one of those rare occasions when it needs to happen.
Need to be very careful using mandates… I think there is real potential to do more harm than good in the long term… outside of very specific circumstance im against.
For example you can argue that institutionalized racism which already see's worse outcomes for both Maori and Pacific people in our society leads to distrust of govt and a reluctance to engage… going down the path of wide spread mandates would potentially further alienate these groups particularly I suspect in the younger age range say 15-25 which long term will probably leave us worse off as a nation you could also argue it would be an extension of the institutional racisim we see in our health and justice statistics already. Waitangi tribunal claim perhaps?
Better to use carrots and if a stick is necessary maybe wave it at someone like Brian Tamaki…
Wait for ACC, Worksafe, Director obligations, Southern Cross, and the main business insurers to make their views known to government. Then come the bank mortgage loan conditions.
Won't be any escaping differential premiums.
This will be way worse than smokers.
Its a very specific circumstance Cricklewood.
And suggesting a similarity to institutionalised racism is a false equivalence imo.
Racism is a disorder that has existed since forever and involves a significant portion of the population. Anti-vaxxers only comprise a tiny percentage of the population but they are vociferous, very aggressive and are attempting to derail a world-wide effort to contain a pandemic. In some cases they are doing it for pecuniary gain. They are not afraid to adopt tactics which in other spheres of activity would attract the attention of law enforcement agencies anyway.
Im not talking about anti vaxxers im talking about the reluctant, those in our society that get the short end of the stick ie more likely to be arrested, more likely to be in unstable or overcrowded housing, etc etc… and these pre existing circumstances which some put down to institutional racism result in a reluctance to engage with the 'system' for the 'public good'.
My arguement is that further marginalization of these cohorts in our society will be vastly counterproductive it needs to be all about the carrots.
I did separate vaccine hesitant from anti-vaxxers in my original comment @ 4.
It should just be your civic duty, right? We don't excuse those who are outside the tax system. They are classed as a "risk to the economy".
Similarly, the unvaccinated are a risk to the health system. They will begin to clog up hospitals in the coming months, taking beds away from vaccinated people who require emergency, medical or surgical treatment. People who have done their civic duty.
By removing vaccine passports from the table, and the possibility of regulations for the workplace and large social events, you give anti-vaxxers and the vaccine hesitant an out. They will take it.
That leads to lower rates of vaccination. Best to keep the pressure on with both incentives, and conditions.
Same wave-length.
Unvaccinated need to be down the hospital lists if there is a need for vaccinated who need hospital care.
“Unvaccinated need to be down the hospital lists if there is a need for vaccinated who need hospital care”
The way our health system works, or certainly here in Welly I believe, unvaccinated non-Covid cases are quite likely to go to the front of the queue because their overall medical risk is perceived to be greater.
The hospital would take any opportunity presented to vaccinate them at the same time.
Which works until the system gets overloaded, then the sickest people get pushed to the "no treatment" area so people with a better chance of survival can be treated.
But triage generally doesn't involve whether the injury was caused by one's own stupidity or a noble accident (medics are human, but they still usually do their job reasonably well).
The incentives are more likely to attract those in difficult situations, and people need reassurance when they feel threatened or frightened.
The earlier or later clinics could help those with difficult work times.
The food /food vouchers idea is attractive in such times.
Laying on "free taxi vans" to transport distant families to a pop up bus in their area.
Sporting and pop icons and influencers encouraging the reluctant.
All that should be tried before any mandates. imo
But as a last resort requests to do certain activities will require vaccinations.
Agree with that. Incentives first. The people living outside of society are at once most at risk from Covid, most likely to spread Covid, and most likely to reject vaccination.
Point I'm trying to make is that by attacking the possibility of mandates and regulations you fuel the real problem, anti-vaxxers, who are motivated to spread fear in the communities referenced above.
You & Patricia both make good points, imo.
All out incentivising & the employment of several different strategies to make actually getting vaccines easier for the hesitant first – but with the legal work done now to provide for mandatory vaxing (and/or exclusion from certain places or activities) so these moves are already legally available when & if required to deal with the anti-vaxers.
Citizens need to take responsibility themselves, not just leave it to “the authorities”.
Ask re vaccination status if someone enters your home, or personal space. I have no compunction in sending friends, acquaintances or strangers packing until they have had shot #1.
Ethnic groups are being supported to deal with their specific vaccination situations, and sub cultures and off grid people need the same active support and encouragement approach. If it takes goodie bags and rewards it is worth it.
40 years of Neo Liberal individualism, and “anything can mean anything” post modernist philosophy have helped get us to this position of over tolerating people that put themselves and others at serious risk.
has anyone found a satisfactory answer from antivaxers about the following scenario. I am not meaning those who do not believe covid is real, obviously they won't contract the virus and get ill. But the antivaxers who rely on their own immune system to protect them.
When an antivaxer gets covid of course their immune system will confer a degree of protection when they recover. However what if they get really ill to a level requiring medical treatment. I assume such antivaxers will do the honorable thing and stay at home and tough it out, rather than fill up our hospitals. If they don't die then they are fine.
The important piece of information here is that pretty much all existing vaccines provide high protection against getting really ill and death. Some are effective against catching the virus however even the weaker vaccines have 80+ protection against serious illness, so low chances of you ending up in ICU after vaccination.
Just been reading SMH item on vaccine passports for Sydney and parts of NSW which are being planned. Pubs, restaurants and hairdressers will be allowed to open for those fully vaccinated after NSW hits 70 per cent vaccination of those 16 and over.
Excellent idea which hopefully will be brought in here. Anti vaxxers don't have any right to endanger others, regardless of their so called rights. Remember the objections to no indoor smoking rules? Who would want to go back to the days of unpleasant smoke from others putting people at risk. As a COPD person who has never smoked, I was told I grew up at a time where everyone around smoked everywhere.
The idiots rioting in Melbourne and Sydney are the ones who will spread and get Covid.
The unvaccinated are far more at risk than everyone else. Your claims that unvaccinated people are putting everyone at risk are quite dubious. If the Sydney plan goes ahead then the 70% of people will be introducing the risk of a large outbreak there.
I wonder what percentage of the First People of Australia have been vaccinated?
Last I looked – similar to NZ.
Restrict access to government services. Suspend driver licences, suspend benefits, suspend tax exemptions, suspend Covid support payments to those who refuse to be vaccinated. Give them plenty of warnings and time to comply. But let them know that it is not acceptable to pose a public health risk because of some shit you read on Facebook
The messaging has to be way clearer and better than for mask use. At this time in several instances people who got a mask exemption and followed all the rules were still discriminated against. There are a small number of people who can't be vaccinated so the govt policy will need to have and work with occasional exemptions.
Roblogic, that would just push some communities further away. What about their children? They would be collateral damage, and such policies reek with Big Brother overtones.
Community and Public Service means helping when people are marginalised by poor health poor education poor housing rubbish food and ease of access to mind numbing lies on some internet platforms.
They need support to think this through with a view of a better future. Hope not threats.
The group who should be tackled are the spreaders of misinformation. Fines, community service etc.
Good post mickey. I'd like to see the msm stamp on any conspiracy antivaxer dog whistling (hello Judith).
Oz have 2 MP's spreading such that scumo and Barnaby refuse or are unable to reign in.
We need to make every effort.
A lot of people are realising what it means to be outside the economy and society now. No wage subsidy or RSPs for you if you haven't been paying GST.
Same should go for this particular health initiative.
All sounds a bit tribal to me – let's drive those that are not like us OUT!
My prediction is that this is not going to end well and may well degenerate into extremes of violence.
I sincerely hope not.
A pleasantly balanced post
Just a couple of dissenting thoughts.
The narrative has radically shifted from the start of the pandemic. Cousin of the common cold, can't vaccinate for that. 2 years later, the drums are beating for compulsory medication
This enthusiasm for mandating medication, does this apply to boosters, 'next generation' vaccines etc. If so, get yr Big Pharma shares now.
I have heard talk of businesses offering $100-$150 to staff who have been reluctant. Not a lot of money to someone who is reticent.
This seems like the top of a very steep, slippery slope.
A steeper slope is 7000 possible deaths and who knows really, how many hospitalisations ?(Hendy)
Equating vaccine reluctance with “Big Pharma” is a bit of a red herring. We are collectively paying for this from the covid purse, at no cost to the individual, and any notion such incursions are begun to make money is a stretch.
Here's another modellers rebuttal of that number, and Hendy's reply. It's worth noting that the 7,000 claim is based on 'no restrictions'.
Has aroused some stats community chat.
https://twitter.com/tzemingdynasty/status/1440932248912494596
[link fixed]
Thanks – can you repost the link…that one doesn't work.
Thanks Sascha. It seems the model Hendy used has a problem with the vaccine efficacy levels.
It seems you know how to correct this problem, so please don’t hold back and share your knowledge and put it out in the open, just as Hendy and co-workers did. Me thinks you’re just another arm-chair expert and critic who knows nothing much.
I have no idea how to fix the problem. But then I'm not being paid the big bucks to supposedly inform the public. The 7,000 deaths claim has been described by another modeller as “absolutely unconvincing”, and since then there has been criticism of the vaccine efficacy used in the original modelling, and that the model assumes no restrictions. Producing information that has more than an aura of alarmism, at a time when the government is trying to get more people vaccinated, doesn’t seem that helpful.
Intriguing comment.
Do tell.
Do tell again. Any idea if "another modeller" is being paid bigger bucks?
"More than an aura of alarmism", you say. Intriguing again.
Which do you think might be more helpful in persuading Kiwis to get vaccinated: an estimation of the potential deaths should COVID-19 get more than its current toehold among the unvaccinated; or expressions of 'concern' along the lines of "more than an aura of alarmism"?
"Which do you think might be more helpful in persuading Kiwis to get vaccinated: "
Education. Science. Statistics.
“If you’re going to use this model in this way it should be peer-reviewed by global experts. It's absolutely unconvincing – it really needs to be reworked.” Jones said the country didn’t need to be scared into getting vaccinated with talk of high death tolls. “We need a positive story. The evidence is that negative takes and the use of fear does not get people vaccinated,” Jones said."
Absolutely. Is Jones an educator? A scientist? A statistician?
Rodney Jones, MA (Hons) in Economics, BCom. Area of expertise: economic analysis.
Don't know about you or Jones, but NZ's COVID-19 health outcomes to date paint a pretty positive 'story' to this natural pessimist.
https://www.worldometers.info/coronavirus/country/new-zealand/
https://www.theguardian.com/world/2021/sep/24/jacinda-ardern-looks-to-life-beyond-lockdowns-with-90-vaccination-target
https://www.scoop.co.nz/stories/PO2109/S00151/new-zealand-government-eases-covid-19-lockdown-in-auckland.htm
http://www.news.cn/english/2021-09/24/c_1310206413.htm
"Absolutely. Is Jones an educator? A scientist? A statistician?"
I wasn't aware he was now the only communication medium for all of government.
"but NZ's COVID-19 health outcomes to date paint a pretty positive 'story' to this natural pessimist."
Indeed. Which makes the alarmist claims about 7,000 deaths all the more unhelpful.
Please show your justification for calling one particular value in Hendy's document "alarmist". What number does your modelling show for the same assumptions?
Gypsy, you linked to economist Jones' critique @15.1.1 (6:18 pm), and quoted Jones @7:03 pm. Do you perhaps, like “another modeller” Jones, believe that the predictions from scientist Hendy's modelling are alarmist? Because that’s the impression I’m getting.
If Jones believes "we need a positive story", how about: Since March 2020 New Zealand has recorded 408 days of ZERO community cases. A well-deserved reward for some hard work by the team, imho.
https://www.covidplanb.co.nz/our-posts/dissection-of-prof-hendy-model-presented-at-ardern-conference-23-9-21/
"Do you perhaps, like “another modeller” Jones, believe that the predictions from scientist Hendy's modelling are alarmist?"
Do you believe that the documented shortcomings in Hendy's model are inconsequential?
“A well-deserved reward for some hard work by the team”
The reality of what we have achieved and the mitigation measures used, seems to make a nonsense of using a model that assumes we won’t use the full mitigation measures we have available. Agree?
It was a straightforward question Gypsy, but I can understand why you'd rather not answer.
I'm OK maintaining previous "full mitigation measures" indefinitely – are you?
For better or worse, "full mitigation measures" aren't set in stone; new COVID-19 variants, increasing vaccine coverage, the capacity of the public health system, and team acceptance of those same measures are just some of the continuously changing inputs that affect a modeller's predictions.
Time will be the best judge of worth of Hendy et al.'s modelling, and far better than ‘judge Jones’, imho.
" I can understand why you'd rather not answer."
Except that I already had.
“”full mitigation measures” aren’t set in stone; ”
That’s no excuse for leaving them out.
If you say so – perhaps the reviewers will insist on putting them in.
Some seem to be fixating on the predicted worst outcomes (which "could be mitigated if more restrictive control measures, akin to current Alert Levels 3 or 4, were utilised.") in just one of several alternative scenarios analysed by the team of modellers.
The last three bullet points in the executive summary, which include the offending "7,000 fatalities per year", seem realistic rather than alarmist, but then we all have different ‘alarm thresholds’ on any given topic, and that could explain your 'concern'.
https://www.worldometers.info/coronavirus
Modelling to support a future COVID-19 strategy for Aotearoa New Zealand [Steyn Plank Hendy, 23Sept 2021; PDF]
• We find that there are scenarios where, through a combination of high vaccine coverage (including amongst those aged 5-11) and moderate public health measures, population immunity is achieved, resulting in very low mortality burden. For example, with 90 per cent vaccine coverage of the population over the age of 5, a suite of moderate public health measures and an effective test, trace and isolate system, the modelling suggests there would be around 500 hospitalisations and 50 fatalities from COVID-19 over a one year period.
• There are scenarios where, despite a high vaccination coverage, population immunity is not achieved, resulting in a disease mortality burden that is an order of magnitude greater. For example, with 80 per cent vaccine coverage of the population over the age of five and moderate public health measures, the modelling suggests there would be around 60,000 hospitalisations and 7,000 fatalities per year from COVID-19. Such outcomes could be mitigated if more restrictive control measures, akin to current Alert Levels 3 or 4, were utilised.
• Nonetheless, the results suggest that a combination of high levels of vaccination within the community, a strong test-trace-isolate-quarantine system (assuming case numbers are kept sufficiently low) and moderate public health measures may be enough to attain population immunity, greatly reducing the need for strong public health measures, such as stay-at-home orders and workplace closures.
"Some seem to be fixating on the predicted worst outcomes…"
Understandably, given those are what Hendy is emphasising in the media.
"The last three bullet points in the executive summary, which include the offending "7,000 fatalities per year", seem realistic rather than alarmist…"
I tend to distrust those numbers on a mathematical basis, using hospitalisation and mortality data I have posted here previously.
"Not following that answer."
Nor do I! I meant to say "to regain some kind of normality". I'm pro vaccination, and believe a high vac rate is the best way to mitigate the ongoing financial and social cost of Covid.
Yep, agree with that.
Both of Sweden's pre-vaccine COVID waves peaked at ~100 deaths per day. Fortunately for Kiwis, our government followed the prudent advice of health experts and implemented precautionary measures to limit the freedom of the virus to infect and cause illness/death.
I'd prefer that most things went back to 'normal' sooner rather than later, and I'd prefer even more to continue following the advice of health experts that have served us exceptionally well to date, because I believe that’s the best path for NZ to get back to ‘normal’ with minimal loss of life.
In this pandemic, a little public patience is not just a virtue – it can be a lifesaver. Imagine if we'd had to wait years for an effective vaccine.
Heard on the radio the other night that six vax buses have been on the road for a week and have only vaccinated 400 people! That's very disappointing if true as that is less than 10 people per day per bus!
And folks were "disappointed if true" when the main vax rollout was just beginning, as well.
Does "on the road" mean "fully staffed, equipped, and operational, and parked in a major centre's supermarket carpark with full advertising"? Or does it mean "couple of days to get the crew to familiarise themselves with it, and then a tiki-tour around some remote small communities do get rural people vaxed and test out the routine"?
As suggested, perhaps parking one next to the KFC drive through would up the numbers.
or perhaps there isn't a KFC where the buses have been operating. Remote people need jabs, too.
"Shot Cuzz will be parked at the Clendon Park, Pak'nSave car park this Tuesday and Wednesday and Southmall, Weymouth Rd entry, Thursday and Friday from 9am to 4pm."
It's not that remote if there's a Pak n Save there!
https://www.nzherald.co.nz/nz/covid-19-delta-outbreak-new-vaccination-bus-shot-cuzz-hits-auckland-streets/JZMDL3PD6S7CDWOFAOREV2TWMY/
So is that bus number 7? When did the other six start, and where?
Do you know the difference between remote and hard-to-reach communities/sub-populations?
You’re repeating the same lie again that one of Hendy’s many (!) predicted outcomes (i.e. your all-time favourite of 7000 deaths) was the worst case scenario when i
Except I didn't use the figure of 7,000 in that comment, did I?
[Which number AKA worst case scenario did you have in mind, this time?
You’re wasting my time, and McFlock’s, but he seems to be still enjoying it (!?), so you’d better make it work well for you because I’ve lost my patience with you a while back. The only reason you’re hanging on to your commenting privilege is that this is an older Post – Incognito]
See my Moderation note @ 5:03 pm.
I disagree with you, but I respect the role of moderator, so I will disengage.
Not lying repeatedly helps.
I wouldn't know.
Don’t worry, the Moderators can and will tell you. Take heed and you’ll be ok.
Edit: good edit, BTW.
Thanks. I'm trying to be good.
It's getting towards the end, but there's a sort of graceful symmetry when they start finding the limits of their inventiveness – I imagine the threads like a linear flow chart that slowly turns into a spiralgraph sort of thing, with loops and swirls and eddies as they recycle points from earlier in the thread.
Sometimes the painting is finished when every comment can be responded to with a sequence of links to earlier comments (preferably theirs).
Sometimes it just fnishes when the computer finishes counting whatever I'm counting and I can start outputting the pretty charts and tables, and no longer need a low-cpu distraction to keep me awake (it's embarrassing when a colleague wakes you up and the computer finished counting an hour before)/
"Please show your justification for calling one particular value in Hendy's document "alarmist"."
It isn't peer reviewed.
It "didn’t pass the “plausibility test” when compared to real-world results in other countries."
“It's absolutely unconvincing – it really needs to be reworked.”
The report is "overcooked" and "rushed"
"It had the feeling of being rushed out with a sensational number,"
The model is an "artificial construct" .
The model assumes only baseline public health measures and limited test-trace-isolate-quarantine
It's sensationalist, and not helpful.
Jones' arguments aren't peer-reviewed either.
All models are constructs. As an economist Jones should know this.
But most of all, I was looking for your thinking on this. But you're just latching onto (ahem) news reports.
BTW, Singapore is back up to a thousand cases a day (h/t advantage) with over a hundred on oxygen last weekend. But then I'm not sure they meet the full criteria of assumptions for the "7000" mark you guys obsess over.
"Jones' arguments aren't peer-reviewed either."
Jones’ isn’t making the claims of 7,000 deaths. He’s critiquing the model, not publishing it.
"All models are constructs."
Yes, but the word 'artificial' was meant to convey the lack of real world reality.
"But most of all, I was looking for your thinking on this."
My thinking is that the 7,000 is hyperbole, based on the current vaccination trajectory, the hospitalisation rate for vaccinated people, and the death rate for fully vaccinated people (around 0.5% of covid patients).
"BTW, Singapore is back up to a thousand cases a day (h/t advantage) with over a hundred on oxygen last weekend."
In 21 months, Singapore has had 70 deaths from 82,860 cases. That's 1 death in every 1150 cases, or 1 death in every 80,000 people. Even using them as a comparison (which is dubious given their population density is around 500 times more than ours), to get to 7,000 deaths with our population would take, well, a hell of a long time. Still, I guess if we wait long enough just about any prediction could come true.
Singapore has had 15 deaths this month, out of their total of 70.
OK, so what are the numbers you are projecting for vaccination coverage and disease control measures?
The worst-case 7,000 figure was an example for 80% vaccination (>=5yr) but community exposure with no measures beyond level 2 (i.e. no L4, no L3 stay-at-home orders) and limited TTIQ.
That becomes 50 deaths at 90% fully vaccinated and full TTIQ.
Should we read that you are expecting a rate of fully vaccinated people five and over being in excess of 90%? Are you assuming higher vaccine efficacy than Hendy's model?
Are you even disagreeing with the model, rather than just the worst-case scenario paragraph from the executive summary (ignoring the better case scenarios in the same section)? Have you even read the report? There's a link to it in comment 22.
"OK, so what are the numbers you are projecting for vaccination coverage and disease control measures?"
I'm not 'projecting', but my gut feel is there will be around 10% of the population who are anti-vac or vaccine averse/hesitant. I'm also of the view that a lot of parents will not want their 5-12 year olds vaccinated.
"The worst-case 7,000 figure was an example for 80% vaccination (>=5yr) but community exposure with no measures beyond level 2 (i.e. no L4, no L3 stay-at-home orders) and limited TTIQ. That becomes 50 deaths at 90% fully vaccinated and full TTIQ."
The deaths number 7000 is mathematically implausible, based on the known data around cases and mortality.
"Are you even disagreeing with the model, rather than just the worst-case scenario paragraph from the executive summary (ignoring the better case scenarios in the same section)? Have you even read the report? There's a link to it in comment 22."
Yes, i have read the report. Yes I understand the 7,000 was a worst case scenario. I do a lot of business scenario modelling, and I would never present a paper to shareholders that was 1) not peer reviewed and 2) not plausible given other known factors.
So if you have access to the report, and all the workings are in the report, what bit of the report leads to the worst case scenario being too extreme, according to your gut?
It seems that your gut feels tell you that vax uptake will ballpark 90% and therefore the 80% bound is unrealistically low. Is that it? Is 80% completely impossible, though?
Here's how I think it will play out – the adult population will get to around 90%, the under 12's nowhere near that, maybe 66%.
But that doesn't paint the full picture. I expect the vaccine uptake by the more vulnerable to be high, so while cases will continue, the death rate will be low.
The death rate in the general population globally is around 0.1%. The death rate from the current outbreak in Singapore is 0.18%, say 0.2%, with 80% of their population fully vaccinated.
On that basis, for us to get 7,000 deaths, say over 2 years, we would need a population of 17.5m.
The death rate is around 2% of the total number of cases.
On that basis, for us to to get to 7,000 deaths, say over 2 years, we'd have to have a total of 175,000 cases.
Assuming my maths is correct ( ), and acknowledging the 2 years is arbitrary, the 7,000 number doesn't pass any kind of reasonableness test.
), and acknowledging the 2 years is arbitrary, the 7,000 number doesn't pass any kind of reasonableness test.
So for a start, that's ~87% vax estimate. Not 80%. Hendy didn't project 7000 dead for 87%.
Secondly, the death toll is projected for one year from the first case of an outbreak, not 2.
Thirdly, that leaves half a million eligible people unvaccinated. Even if only a quarter of them catch it, with your 2% CFR that's a couple thousand dead right there, at 87% vaccination.
"So for a start, that's ~87% vax estimate. Not 80%. Hendy didn't project 7000 dead for 87%."
Even at 8-%, the numbers don't add up.
"Secondly, the death toll is projected for one year from the first case of an outbreak, not 2."
Which makes the numbers even more absurd. To have that many deaths with our population would mean 350,000 cases out of a population of 4.917m, which is 7% of the population.
"Thirdly, that leaves half a million eligible people unvaccinated. Even if only a quarter of them catch it, with your 2% CFR that's a couple thousand dead right there, at 87% vaccination."
In 2020 we had level 4.
A quarter might be high, but 1 in 8 yanks have been infected. So let's halve that, 1/16, and take your revised death rate of 1.15%. That's about 420 dead.
So you'd be able to precisely describe the exact errors in the report for 80%, and what the true value should be.
"In 2020 we had level 4."
Not the whole year we didn't.
"A quarter might be high, but 1 in 8 yanks have been infected."
But not 1 in 8 kiwi's. In the period before vaccinations, the infection rate in nz was 0.04% or 1 in every 2,500.
"So you'd be able to precisely describe the exact errors in the report for 80%, and what the true value should be."
That's for Hendy to resolve. He needs to explain why his modelling produces results that defy all mathematical reason.
We had L4 for the times we had covid in the community. That is why only a couple thou NZers have had covid by now, not an eighth of us. [edit: or do you think NZers have a natural immunity to covid19 that we can share with the rest of the world?]
Well, given that your projection for 87% >5yo vaccination results in 420 dead, and his projections for 85 & 90% are 1411 and 50 (respectively), you both seem to be in the same ballpark.
His only sin seems to be to have applied that math to vax levels in the 70-80% areas for different eligibility requirements. Do you think Hendy should not have presented the calculations for 70-80% vax rates?
Me, I like it when I get presented a range of options upon which to base a decision. Even the unrealistic options, so if someone asks a stupid question I can say why it's stupid (in a considerate and inclusive way, of course).
"Me, I like it when I get presented a range of options upon which to base a decision."
Sure, but I'll go back to my business example. The range of options still need to be within the realms of mathematical believability. I don't think Hendy's are. But we can agree to disagree.
So you don't think NZ levelling off at a 70% or 80% vaccination rate isn't mathematically believable?
Or do you think there is something weird about NZ that reduces the R0 of covid19 to a fraction of it's level overseas?
You're not actually making any statements to agree or disagree with. You think Hendry's worst case scenario is unrealistic. Well, it's possible, but it's a worst-case scenario, if it turns out that a fifth of the country get persuaded to avoid vaccination. I hope it's unrealistic, because your opinion seems to be consistent with his math in the 85-90% modelling ballpark.
But I don't think it would be appropriate to just assume a mid-case or best-case scenario will eventuate.
"So you don't think NZ levelling off at a 70% or 80% vaccination rate isn't mathematically believable?
I don't think the predicted outcomes are mathematically possible, given historical infection and mortality rates. A peer review would have asked those questions and resolved them.
Except you haven't raised any questions. You just say you don't like the numbers.
And using your own mortality figure, the 87% >5 vax rate has a mortality between Hendy's projections for 85% and 90%. So at least for the range of vax you find likely, his results aren't "mathematically impossible".
Perhaps you don't like the baseline R0 for delta: 6. What value do you believe it should be?
Do you think his range of estimates for pfizer effectiveness are far too low? Why?
Sure, the math for low achievement is scary, but it's backed up by experiences overseas.
I’m not saying I don’t ‘like’ the numbers. I’m saying mathematically they make no sense.
1. The NZ Population is 4,917,000.
2. Hendy uses a Vac rate of 80% for over 5’s. let’s use 70%.
3. That leaves an unvaccinated population of 1,475,100.
4. In 2020, NZ had 2174 infections across an unvaccinated population. That is an infection rate of 0.0442%.
5. Apply 0.0442% to the unvaccinated population (1,475,100) and the result is 652 infections.
6. The case fatality rate for NZ is 0.65%.
7. That’s 4 deaths.
Seriously??
Your comment has more holes than a Swiss cheese skewered by Sir John Key at a cheese fondue.
You think Hendy should assume that a population without level 3 or level 4 movement restrictions would have the same infection rate as a population that shut down entire sectors of its economy for months (and told people to stay at home for all but the most essential reasons for weeks)?
Please, go into more detail on that. I would love to know how months of lockdowns don't affect the infection rate of a communicable disease.
"You think Hendy should assume that a population without level 3 or level 4 movement restrictions would have the same infection rate as a population that shut down entire sectors of its economy for months (and told people to stay at home for all but the most essential reasons for weeks)?"
I think Hendy should assume that the government would apply lockdown's consistently. And done some maths. To get to 7,000 deaths on those numbers would require an infection rate of 75%.
McFlock here’s a variation on my original calculations using global data for Infection rate at 2.8538%, and Case fatality rate at 2.05%.
Number of deaths 863.
I think that various projections should include the full range of options being discussed by NZ politicians and public figures, including the leader of the opposition saying L4 wouldn't be necessary with 70% vaccination of 12+.
National ranges within that global infection rate being from 0% to something like 12.5%.
So, zero, no worries.
But 1/8 of those 1,475,100 is 184,387 infections and 3,600 dead.
It would be great if it was zero, but I'm not going to bet nan's life on it.
"I think that various projections should include the full range of options being discussed by NZ politicians and public figures, including the leader of the opposition saying L4 wouldn't be necessary with 70% vaccination of 12+."
OK, but the current government is in power at least until late 2023.
"National ranges within that global infection rate being from 0% to something like 12.5%. So, zero, no worries. But 1/8 of those 1,475,100 is 184,387 infections and 3,600 dead."
Yep, but then you'd have to almost double the mortality rate to get to 7,000 deaths.
Anyway, thanks for the discussion.
Are you suggesting that Hendy shouldn't consider the full range of options in the public discussion simply because our government can do what it wants until 2023?
So? Being off by 2% isn't exactly outside the realms of being "mathematically possible". Treasury forecasts routinely fail by more than that, particularly in election years:
Maybe rather than having economists expounding forth upon epidemiological predictions we should have health researchers doing economic projections.
Are you suggesting that Hendy shouldn't consider the full range of options in the public discussion simply because our government can do what it wants until 2023?
No, I’m suggesting any modelling should take into account the track record of the current government.
So? Being off by 2% isn't exactly outside the realms of being "mathematically possible".
It's not 2%. To get to 7,000 deaths, you have to assume an infection rate 280x what we have experienced (from 0.0442% to 12.5%), and a mortality rate 4x our historical experience and double the world average. Or a combination of those.
There are very few countries in the world with a mortality rate from confirmed cases above 4%.
Doesn't that do the country a disservice? What if collins were right and 70% was sufficient vax level to keep deaths to a minimum? Shouldn't Cabinet and the country be made aware of that? And shouldn't the Cabinet and the country be equally made aware that the data doesn't fit Collins' complacency?
Dude, enough with the 0.0442% bullshit. We're talking about doing without L3 and L4, not jumping the nation to L4 if there's a single covid-positive case.
So it's not just mathematically possible, it's actually happened.
Doesn't that do the country a disservice?
No. Go back and review the level of intervention built in to Hendy’s model and compare it to your Çollins’s cenario.
Dude, enough with the 0.0442% bullshit. We're talking about doing without L3 and L4, not jumping the nation to L4 if there's a single covid-positive case.
The 0.0442% is what actually happened. But hey use the world average infection rate of 2.8538%. You still need totally unrealistic variables to get to 7,000 deaths.
So it's not just mathematically possible, it's actually happened.
One variable. For a handful of countries out of hundreds. Now add all the others and you’ll see the 7,000 is not credible.
lol you'd better hope that not wanting to discriminate against unvaccinated people (i.e. vaccine passports) doesn't negate having L3 as an option, because at 70% 12+ the numbers are even worse.
And I'd still like to know how months at level 4 didn't impact our covid transmission rate, according to you.
But hey, you're now including in your global rate populous countries that took extreme measures to control covid, as well as populous countries that might be underreporting their death toll by 90%.
Personally, I'll go with the guy who accurately predicted our actual mortality rate given the controls we actually implemented rather than your gut feels and dodgy math.
“And I'd still like to know how months at level 4 didn't impact our covid transmission rate, according to you.”
I’d like to know why you and Hendy would assume there’d BE no level 4.
“But hey, you're now including in your global rate populous countries that took extreme measures to control covid, as well as populous countries that might be underreporting their death toll by 90%.”
Only for one calculation. Feel free to come up with your variation that shows 7,000 deaths. Your assumptions would have to be heroic.
“Personally, I'll go with the guy who accurately predicted our actual mortality rate given the controls we actually implemented rather than your gut feels and dodgy math.”
You mean the guy who predicted one scenario with 80,000 deaths? That's 2% of our population! Geez that's 11 x what happened in Sweden!
Stop the press: I think you might have made an actual specific challenge to an assumption in Hendy's analysis: you believe that outbreaks would be combatted in the same way as the last 18 months, nationwide lockdowns at one case in the community.
So why are we vaccinating?
Sweden actually implemented some (half-arsed) controls in 2020. So yes, I mean the guy who accurately predicted what happened in reality.
"So why are we vaccinating?"
Because people who are vaccinated still get covid.
"Sweden actually implemented some (half-arsed) controls in 2020."
Half arsed is right. And got not within a country mile of that mortality rate.
Not sure that follows.
But came pretty close to the lower end of options that are similar to what they actually did implement. About twice his estimate for "Case isolation, household quarantine, and population-wide social distancing"
They kept schools open, but "encouraged" social distancing, lots of people self-isolated, and so on. 14,000 dead in 10 million.
But I guess that's mathematically impossible, too.
Not following that answer. Vaccination against COVID-19 decreases the risk of serious illness and death due to infection, with the added benefit of decreasing the chance of infecting others.
Alberta, Canada: population 4.5 million (over half concentrated in two metropolitan areas centred on Calgary and Edmonton); ~80% white; good public health infrastructure; politically conservative.
Sweden had an infection rate of 11% of total population, a death rate from cases of 1.29%, and a death rate to total population of .144%.
Apply those stats to the NZ population and the 80,000 death estimate is out by a factor of 11. It's not even close.
Is the average life expectancy of Māori and Pacific people in Sweden also many years shorter, as is the case in Aotearoa-New Zealand?
so you're saying that Sweden got within a factor of eleven of the theoretical do nothing / change nothing logical baseline for covid responses, while we took the most extreme option modelled and achieved a result that would require a factor of three hundred to match Sweden's deaths, and your takeaway is that the modelling is wrong because no accurate model could have an elevenfold difference between real-world results?
"…your takeaway is that the modelling is wrong because no accurate model could have an elevenfold difference between real-world results?"
If you're ok with an 1100% difference then that's up to you. Given that was early in the life of the Covid experience (March 2020) we can cut him some slack, but it makes the heroic claims in the latest model even more inexcusable. That's why peer review is helpful.
The actual difference between NZ and Sweden's death tolls is 27 times the theoretical difference between the death toll Sweden actually achieved and the "do nothing / change nothing" projection for NZ.
Peer review ain't going to change that.
"The actual difference between NZ and Sweden's death tolls is 27 times the theoretical difference between the death toll Sweden actually achieved and the "do nothing / change nothing" projection for NZ."
The difference between the modelled NZ death rate and the actual death rate in Sweden was a factor 11. No matter how much you try to spin it, a peer review would have picked up the mathematical absurdity of the 7,000 deaths prediction. The data around case numbers and mortality, local and global, would have shown up to any reviewer that the prediction of 7,000 deaths was, at best, hyperbole.
Which is small compared to the real-world range of mortality, and should of course one would expect Sweden to have a lower death count than the "do nothing, change nothing" scenario simply because they actually did some things and some people did change their behaviour.
A ferrari can be outrun by a mini if the mini is flooring it and the ferrari is half-arsing it.
The model is fine. You have a problem with one of the assumptions around controls, yet that assumption (rule out lockdowns) is a recurring part of the public discourse, so it is proper to include those assumptions in that model.
I look forward to see you lobbying for lockdowns now and in the future. Should we be at level 4 right now? What does your modelling suggest?
“Which is small compared to the real-world range of mortality”
The world has a total population mortality rate of 0.059%.
Iceland has 80% vaccinated and has a total population mortality rate of 0.01%.
Denmark has 75% vaccinated – population mortality 0.046%.
Ireland has 74% vaccinated – population mortality 0.105%.
And that includes deaths from before those countries had any of their population vaccinated.
At 80% vac rate, and the 'real world experience' for both cases and mortality, a prediction of 7,000 deaths is not mathematically sound.
“You have a problem with one of the assumptions around controls, yet that assumption (rule out lockdowns) is a recurring part of the public discourse, so it is proper to include those assumptions in that model.”
It's not the assumptions I have a problem with. The model produces predictions for deaths that are mathematically absurd. When the estimate of deaths popped out of the model, that should have been reviewed.
Let’s compare apples with apples and Delta with Delta.
Denmark, for example, has just over 75% of its population fully vaccinated, which means about 90% of its eligible people aged 12+ if their age distribution is similar to NZ (I can’t be bothered checking this, but it won’t be miles off, I reckon).
They have recently lifted most but not yet quite all domestic restrictions.
The 7-day average of daily new cases is ca. 350.
The 7-day average of hospitalisations is just over 100.
The 7-day average of patients in intensive care is ca. 25.
The 7-day average number of daily deaths is between 2 and 3.
The recent modelling by Te Pūnaha Matatini for 90% vaccination of 12+ population, i.e. ca. 76% of total NZ population, predicted 21, 1557, and 6623 deaths over one year in NZ with High, Central, and Low vaccine effectiveness estimates (assumptions), respectively. Although it would not pan out this way during an outbreak, as per the model, 1557 deaths averaged over one year equals just over 4 deaths per day.
Given that NZ demographics are different, e.g. we have a high percentage of Māori and Pasifika people who are more vulnerable and at higher risk of dying from Covid-19, I think the modelling predictions for NZ look eminently realistic to me.
Except your numbers for 87% produced a result between Hendy's 85% and 90% projections.
You then said that the assumption of no level 3 or 4 was what was unrealistic. Now you don't have a problem with the assumptions.
Make up your mind.
“Except your numbers for 87% produced a result between Hendy's 85% and 90% projections.”
“You then said that the assumption of no level 3 or 4 was what was unrealistic. Now you don't have a problem with the assumptions.”
You're getting confused between the inputs and the controls. I have never expressed doubt about the control assumptions. I have been very clear that it is at the extreme high end of the model that Hendy has it wrong. Not because of control assumptions but because his input data for infection rate and case mortality rates (at 80% vaccination rate) do not match real world data.
So you're happy with the assumption that L4 and L3 will not be used under a high vaccination rate?
"So you're happy with the assumption that L4 and L3 will not be used under a high vaccination rate?”
Yes. If I’m challenging the models output, I need to use the control assumptions consistent with that model for that output.
Then why do you insist on using NZ infection and mort rates from last year and this year, when L3/4 were the main tools for infection control?
"Then why do you insist on using NZ infection and mort rates from last year and this year, when L3/4 were the main tools for infection control?"
Fair question.
By how much? It's highly unlikely they'd be an exact substitute, one for the other. I also note that assuming no L3/4 is the exact opposite of what you wrote in the discussion here:
But now you're okay with that assumption, we can move on. You're using L3/4 transmission rates because you believe L3&L4 to have an effectiveness equivalent to vaccination.
So is therefore likely a massive undercount of identified cases and includes data from countries that used measures even more restrictive than NZ. China alone would skew your stats.
Let's go back to first principles: what's your R0 for delta?
How is that R0 affected by moderate mitigation measures – L1/L2, tracing, isolation of cases and contacts, etc?
What vaccine efficacy are you going with?
How do your values for any of these numbers differ from Hendy's?
"So is therefore likely a massive undercount of identified cases and includes data from countries that used measures even more restrictive than NZ. China alone would skew your stats."
Sure. But then the stats also include a significant period when no-one within the population were vaccinated. There is also the possibility that in some countries the death rate has been overreported in situations where people died WITH covid as opposed to OF covid.
"Let's go back to first principles"
Yes, let's. I've made it clear I'm not questioning any of Hendy's assumptions, because I'm not creating a new model. I'm applying a mathematical 'sanity test' to a particular output from the model, using real world historical data. Hendy may well have done the same thing and been satisfied with the variation.
Fixed it for you.
"I'm applying a mathematical 'sanity test'…"
There is no 'gut feels' at all, just maths and actual historical data. It's not like I'm the only one querying Hendy's outputs.
No gut feels, except for your estimate of likely vaccine coverage.
edit: I’ll also point out that while you and one or two others throw shade at Hendy’s report, none of you actually point out (let alone resolve) exactly where Hendy’s model falls down. Sure, you’re an internet whatevs, but Jones could literally peer review it himself, argue about the vaccine efficacy or R0 inputs that lead to the outputs that he has a problem with.
But for some reason the extent of that peer’s “review” is to complain peers haven’t reviewed it.
"No gut feels, except for your estimate of likely vaccine coverage."
Which had absolutely nothing to do with the maths. In fact that comment starts with “I’m not ‘projecting…”. But you knew that eh.
But that's the problem you've created for yourself: you say that Hendy's projections are not mathematically possible, and when asked for the math that leads you to this conclusion you come up with utter bullshit and biased assumptions – like L3/L4 reducing infection rates in precisely the same proportion as NZ's eventual vax rates and vax efficacy.
But when challenged on that math, you're "not projecting" and suddenly the numbers upon which "not mathematically possible" are based disappear.
If you can demonstrate his numbers are shit, fine. But every time you get called on your own working, suddenly you're not providing any basis upon which to criticise the work.
"and when asked for the math that leads you to this conclusion you come up with utter bullshit and biased assumptions"
I'm using a mathematical approach that incorporates real world historical data. The only 'assumption' I'm making is that that data can inform the mathematical calculations. Given that the numbers Hendy claims have been called out by others, I'm in good company.
Assumptions you make include:
There are probably others, but those are more than enough to suggest that your gut feels could do more homework.
"Assumptions you make include:"
No, I'm not making those assumptions at all, and when objections have been raised to the validity of the historical data as a predicter, I've replaced those values with a range of more negative data. Unless you want to take a position that makes heroic assumptions about infection and mortality rates, Hendy's 'worst case scenario' doesn't stack up.
[You’re repeating the same lie again that one of Hendy’s many (!) predicted outcomes (i.e. your all-time favourite of 7000 deaths) was the worst case scenario when it has been pointed out to you that it is not the worst case scenario at all. This is starting to look deliberate and intentional and as wilfully misunderstanding, ignoring, and misrepresenting the work by Hendy et al.
If you must insist, the real worst case simulated outcome in the study is 20,102 deaths (cf. first row of Table 3 in the column with Low VE).
If you keep up with the lies, you’ll know what will happen, don’t you? – Incognito]
Yes, you've become more and more surreal in your efforts to get the result you want.
But if you're not assuming that historical values in NZ 2020 will match the values when covid hits a highly vaccinated NZ, and you're not assuming that the global aggregate values (that run the gamut of responses and reporting protocols) will match the values when covid hits a highly vaccinated NZ, just what values are you desperately cherry-picking now in order to support your predetermined position?
I am beginning to believe your claim that you "do a lot of business scenario modelling". You probably specialise in justifying to managers and clients their already preferred course of action.
See my Moderation note @ 11:29 am.
"You probably specialise in justifying to managers and clients their already preferred course of action."
No, I run an international business. My ability to sniff out bogus data and sanity test outputs from models is part of what keeps producing returns for the people I work for and me in my job.
lol whatevs.
I'm genuinely curious to your answer to this question, though:
I've already answered that.
The only 'assumption' I'm making is that that data can inform the mathematical calculations.
Remember I have flexed those numbers by even higher infection and case mortality rates, and still hendy's number looks suss.
"those numbers"? What numbers are you actually using?
The historical data for infection rate and case mortality rate.
Which historical data? Because apparently you're using neither global aggregate nor NZ data from last year.
"Because apparently you're using neither global aggregate nor NZ data from last year."
That's exactly what I'm using. (I think at one point I quoted the 2020 CMR for NZ at 0.65% (which was actually the total CMR), which I later corrected to 1.15%).
I've just updated the numbers as follows:
NZ
Infection Rate 2020 0.0442%/Total 0.0864%
Case Mortality Rate 2020 1.15%/Total 0.64%
Population Mortality Rate 2020 0.0005%/Total 0.0005%
World
IR 2020 1.06%/Total 2.96%
CMR 2020 2.31%/Total 2.05%
PMR 2020 0.025%/Total 0.061%
So, taking a NZ population of 4,917,00, if we apply the World PMR for 2020 we get 1,200 deaths. To get to 7,000 deaths we would need a PMR of 0.15%, which is x273 the actual historic NZ PMR (both for 2020 and total), x2.5 the total world PMR and x6 the world 2020 PMR.
As you’ve rightly pointed out, there may well be reporting issues with the global numbers, but there are plenty of countries we can trust. For example, the PMR’s for Iceland = 0.010%, Denmark = 0.046%, Singapore = 0.002%, Norway = 0.016%, Australia = 0.005%, Canada 0.074%.
https://www.worldometers.info/coronavirus/coronavirus-death-toll/
https://www.worldometers.info/coronavirus/
https://www.statista.com/statistics/1103040/cumulative-coronavirus-covid19-cases-number-worldwide-by-day/
[headdesk]
So you are making assumptions that:
So now you're in another loop of your own bullshit:
You're assuming the data is relevant to a highly vaxxed NZ population
But
you're not making assumptions that the differences between the historic data and the effects of vaccination are equivalent
Except when you are.
"So you are making assumptions that:"
No, I'm not. You’re first link goes to precisely that comment (“The only ‘assumption’ I’m making is that that data can inform the mathematical calculations.”)
It seems to me you can't actually find a flaw in the maths, so how do you propose we would get to a PMR x273 the actual historic NZ PMR (both for 2020 and total), x2.5 the total world PMR and x6 the world 2020 PMR?
But you denied making that assumption in this comment.
The flaw is in you having a methodology written in preferential quantum mechanics: when a specific aspect of your position is observed, rather than collapsing randomly your superposition collapses in the direction you most prefer at that instant.
"But you denied making that assumption in this comment."
No, I didn't. I'm making no assumptions other than that the historical data is relevant to future predictions. If you want to state that those assumptions are implicit in whether the historical data fits is up to you. Of course you can always try to show how the historical data does not fit.
"…your superposition collapses in the direction you most prefer at that instant."
No, again. Because the argument I'm putting forward is simply that a predicted outcome is substantially at variance with historical data, and, that to arrive at that predicted outcome requires a flexing of the key components that is too large to be viable.
fucksake.
Assuming that you're not expecting me to compare historic data with the actual data from future events, I'll just say that:
Just keep with your circular bullshit. You're assuming the data fits without making any assumption on how very different conditions might or might not affect that consistency? Fair enough. Meanwhile, Hendy let the data form his projections, not the other way around.
Six links to two reports on economist Rodney Jones' critique. Anyone else getting the impression Jones’ critique is being spruiked more than the original modelling?
Hendy's modelling is looking more ludicrous by the hour. And Jones isn't the only one calling it out.
"Immunologist Graham Le Gros told The AM Show on Friday it was "just a model" and "doesn't take into account a lockdown being put on top of that, or if we do booster vaccinations mid-next year, which could really change the game as well".
Thanks for that link Gypsy. I’d just note that Jones and Le Gros haven’t used “ludicrous” as a descriptor of Hendy’s modelling, but you will have your reasons.
""What I think is actually going on is that the modelling is undermining hopes for when things can return to normal and that makes some people despairing and angry. "
I get what Hendy is saying, and he may well be right about some. But that's not where I'm at. I'm concerned that modelling that seems to contain alarmist claims actually undermines the vaccination message, and creates skepticism around the science.
I'm often skeptical of people who are telling me what I want to hear.
What part don’t you understand about hard-to-reach communities?
"I think the modelling predictions for NZ look eminently realistic to me."
The 7 day average daily deaths gives a mortality rate of 0.0189%. To get 7,000 deaths in NZ would need a mortality rate of 0.1424%, a factor of 8 higher than your example, so you seem to have reinforced my point.
You can think whatever you like, but to get 7,000 deaths at 80% vaccination is simply not plausible.
The same model predicts 1557 deaths over a one year-period at a population vaccination level similar to Denmark’s assuming Central vaccine effectiveness. Denmark’s steady stream of Covid-19 deaths, which is not an outbreak as per the model, would add up to between ca. 730 and 1095 deaths over a period of one year. I think that is pretty close to 1557, don’t you agree?
I know you’re trying hard but you’re not making the correct comparisons and assumptions here.
My point has always been to question the 7,000 deaths number (and the earlier 80,000 number), ie the worst case scenarios. The low and mid range scenarios may well be fine.
You can question whatever you choose, but the model/modelling appears sound to me; you simply don’t like the results and you try desperately to find fault with it by making incorrect comparisons and assumptions to confirm your cognitive bias.
Why are you so hung up on that one single predicted number of 7000 anyway? There are whole tables with predicted numbers in the study report, yet you cherry pick that one!? Is it because the media zoomed in on that one too? In which case you’re not very original nor an independent critical thinker, it seems.
With slightly different input parameter values, we go from 1557 to 7004 deaths. Neither is a worst-case scenario, which would be 6623 and 11870 deaths, respectively, assuming Low vaccine effectiveness.
If ca 4 deaths per day seems an acceptable (does it?), as in realistic, model prediction then why is 7000 deaths over one year all of a sudden unacceptable, as in unrealistic and “not mathematically sound”, “mathematically absurd”, “mathematically they make no sense”, “mathematically implausible”, and other emotional outbursts of utter disbelief? You cannot have it both ways.
Please put your IQ to work and come up with a better rebuttal because as it stands, you’re simply wasting your own and our time with frivolous pseudo-analysis.
PS We have dealt with that 80,000 number previously, but if you don’t want to learn anything here then we’re indeed wasting our time with you.
It's really quite simple. Given NZ's population, real world results for infection and mortality, the 7,000 prediction was always mathematically ropey. I've repeatedly evidenced that, and your own example (Denmark) confirmed it, even if only for a 7 day period.
"Why are you so hung up on that one single predicted number of 7000 anyway? "
Public policy is based on these models. They should be peer reviewed, and I’m confident the questions I’m raising would have been asked.
“With slightly different input parameter values, we go from 1557 to 7004 deaths. ”
Not so. The input variables to get to 7,000 deaths in the NZ situation require inputs so far in excess of real world data as to be implausible. That’s the point.
“If ca 4 deaths per day seems an acceptable (does it?), as in realistic, model prediction then why is 7000 deaths over one year all of a sudden unacceptable,”
Because the difference between 1,400 deaths and 7,000 deaths is significant. More than significant.
sigh and groan
I like your word choice “mathematically ropey”, which is a very apt description of your own ‘evidence’ and algebraic acrobatic contortions.
Do you know what a 7-day average is AKA 7-day rolling average AKA 7-day moving average? It seems not.
The Danish actual data are actually quite close to the model predictions for NZ.
The model results inform in different ways then you seem to think. Policies and Public Health measures are not based on a single model prediction and most certainly not on your personal favourite of 7000.
Peer review is not about to change the model predictions to numbers that you find more ‘plausible’.
From the not-yet-peer-reviewed technical study by Te Pūnaha Matatini:
Reference [4] has been peer-reviewed by and published in a top medical/science journal.
For example:
Looks like both studies are quite consistent too.
Edit: you were still editing your comment and I missed your last two paragraphs and you changed some other wording too, I noticed. It doesn’t fundamentally change my reply.
You need to get over your mental block and bias of what you find plausible and implausible; in science you don’t get to pick and choose based on what you like and/or prefer. In non-linear models such as these, a slight change in parameter values can have major impact on output values; this is the nature of the beast and many beasts are exponential or power functions. The term/concept “significant” has a specific meaning in modelling and it is not how you use it.
The danish data is not ‘quite close to the model predictions’ if you're looking at the most recent Hendy model
“Where 0–11 year olds are not vaccinated and total population uptake is 80% (the maximum uptake is 84.9% and HIT [herd immunity threshold] is not achieved) there is an estimated 37,700 total hospitalisations (peak 2,980 active and 343 new daily cases in hospitals), and 3,120 total deaths.”
The hospitalisation rate (1%) is about right, but the case mortality rate is 8x the NZ data and 4x the global averages. Now that there is a problem.
Put simply:
NZ Population is 4,917,000
In 2020, the infection rate across the entire population (all of whom were unvaccinated) was 0.0042% (2,174/4,917,000).
The case mortality was 25 or a case mortality rate of 1.15% (25/2,174).
At 80% vaccination rate, the unvaccinated population is 983,400.
983,000 x 0.0042% = 435 cases.
435 x 1.15% = 5 deaths.
And here's the kicker:
Even if we apply the global infection rate of 2.8538% to the entire NZ population (meaning zero vaccine efficacy), and the global case mortality rate at 2.08%, we only get 2,900 deaths.
sigh and groan again
Wrong numbers, wrong assumptions, wrong conclusions AKA garbage in, garbage out.
Here’s one kicker for you: the Te Pūnaha Matatini study explicitly rules out Level 3 and 4 restrictions. Question for you: how many times did we have these in 2020?
Here’s another kicker for you: the Te Pūnaha Matatini study assumes the following:
Question for you: do these conditions apply to NZ in 2020?
Here’s another kicker for you: the Te Pūnaha Matatini study is specifically for the Delta variant. Question for you: which was the dominant variant in NZ in 2020?
I could just go on, but knowing that you’re identical to a previous commenter here who refused to admit that they were wrong when it was blatantly obvious this was the case, and which ultimately led to a ban, I’ll stop here and now because it gives me no joy banning somebody who so obviously just doesn’t get it. Just be careful that you don’t spread misinformation about Covid-19 vaccination and ignorance is no excuse and wilful ignorance is just irksome.
"Question for you: how many times did we have these in 2020?"
How many people were vaccinated in 2020? None.
The model output we’re focusing on is at 80% vaccinated.
Do you seriously think that with no controls but 80% vaccinated the global average data is not applicable?
What I read is the assumptions and caveats of the Te Pūnaha Matatini study, which you don’t seem to have taken in and/or understood. It models the effects of various levels of controls, it assumes various levels of controls, it is a lot more nuanced than you seem to think and a lot more realistic based on real world data as much as possible, contrary to your belief. Why don’t you read it, let it sink in, and learn something before you comment here and put your biased and wilful ignorance on full display? You know what often happens to people who win millions in Lotto? They think they have won a couple of thousand because they simply cannot comprehend the truth at first. You remind me of those lucky ones who cannot believe their eyes, but in a negative way.
You can’t even answer my simple questions because your bias gets in the way and you know it.
"What I read is the assumptions and caveats of the Te Pūnaha Matatini study, which you don’t seem to have taken in and/or understood. It models the effects of various levels of controls,"
You're totally missing the point.
I'm not arguing the control assumptions. I'm not arguing the caveats.
I'm saying that working WITH those assumptions and caveats, the prediction of 7,000 deaths requires either an infection rate or case mortality rate (or a combination of the two) that is outside of any acceptable deviation from the historical real world data. Now if you disagree, then show me where I've got the actual calculations wrong.
Read the study and the references therein and once you’ve done that and understood all of that get back to us, thanks.
400 more Kiwis vaccinated – outstanding! Keep up the good work.
So, saving lives.
https://twitter.com/zeborah/status/1440895007553032203
Dealing with a covid outbreak with a low-vaccinated population is going to be very difficult to do without extended lockdowns. Lockdowns curtail actual Bill of Rights rights to freedom of movement, freedom of association, freedom of peaceful assembly, freedom of religion.
With a highly vaccinated population, outbreaks can be suppressed with much less restrictive measures that at worst very lightly restrict those rights.
So it's simple, bring on the vaccine passports. Those that value refusing one of the safest, cheapest, lowest risk, most thoroughly tested medical interventions ever devised can live the lockdown life by themselves, not force the lockdown life on to everyone else.
The right to refuse medical treatment does not confer any rights beyond one's own skin. It does not confer the right to be a willful health and safety to everyone around you, whether at work, at the supermarket, at a concert, wherever.
The other thing really needed urgently from this government is clear legislation that "no jab, no job" workplace policies are totally justifiable on health and safety grounds, and that the current circumstances make it totally fine to unilaterally add that in to existing employment contracts.
National still extremely bullish on your application to run the health ministry. In fact keen for you to be responsible for policy in almost any area of NZ life. No need to vote blue, but please contact JC about your part in the National revival.
Since JuDarth is now pandering to anti-vaxers, that's unlikely to be a successful career move.
https://www.newshub.co.nz/home/politics/2021/09/coronavirus-judith-collins-urges-employers-not-to-reject-the-unvaccinated.html
I guess if she's feeling her popularity slip below Billy Te Kookiha's, then that might look like a good move.
Successful career move for who?
National will surely consider how popular your policy measures are before
sacking your ass as a Labour cronyprogressing your career.Maybe Vernon Tava will pop back out of the woodwork. Or Gareth.
Andre, Perhaps that was "the poisoned chalice." Till mentioned.
Although I suspect we will still come out miles on top, it is a little premature comparing death rates. This pandemic still has a long long way to go.
In the next 12 months though we are going to see and feel some of the pain that most of the rest of the world expereinced in 2020.
90% vaccination still leaves half a million of our friends, neighbours, brothers, sisters, colleagues etc unvaccinated. Whatever their reaons are, some of them will get very sick, and some of them will die when we open the doors. There is no way around that.
Yep, will be a reasonably solid number of double vaxxed people fall seriously ill usually older (over 60) and/or with other pre existing issues on top of the unvaxxed.
Am I the only one going hmmmmm at the ongoing stereotyping grouping together of KFC customers and "vaccine hesitants"?
https://www.stuff.co.nz/national/300413828/covid19-govt-considering-vaccinating-people-in-fast-food-queues
Perhaps in Auckland, this the reason to come out.
Nope – you're not the only one.
Also, would eating residual antibiotics or hormones in the chicken (assuming they survive deep-frying and the application of 'secret herbs and spices') be common practice in the chemophobic?
Does anybody know where to find a copy of the Shaun Hendy modelling report?
I think we can get to a good place with encouragement rather than coercion. Peer pressure will help – if everyone at work has been vaccinated and obviously had no serious issue, you start to feel a bit stupid being the only one refusing.
I would reserve coercion for anti-vaxxers – not getting them vaccinated, but public distribution of vaccine misinformation should be criminalised. So putting antivax leaflets in letterboxes, harrassing people outside schools etc should be a crime.
Yes. Said the same thing here the other day. Its the way to go because in the current circumstances it is a crime. No need to use bans. Just prevent them from spreading disinformation. Stops them causing any further damage.
Personally, I don't think there's any need to talk coercion yet.
The low-hanging fruit is done, for the next 10% or so I reckon we'll need the ladders to reach out. Our health inequities bite us in the arse around the mid 80s, and a chunk of folks will grumble but do it when employers start asking (then insisting), and being the odd ones out who haven't done it.
If we look at kids and their vax schedules(p66), we are pretty good at hitting 90%, but the caveat on that is that we miss it dismally at the six month schedule and "hesitancy" is only a part of that (~5% for all reasons). A lot of it is access to healthcare and barriers – not just financial ones, the gamut of socioeconomic inequity, language, education, transport, etcetcetc.
Buggered if I'm going to take L4 as a risk for another 18 months just because we're shit at addressing equity in a timely manner, though.
@ William
https://www.tepunahamatatini.ac.nz/out-and-about/
https://www.tepunahamatatini.ac.nz/files/2017/01/modelling-to-support-a-future-covid-19-strategy.pdf
Thank-You
Mr Parker said Hager had been painted as a villain by the Government after the release of his book and today’s findings vindicated him.
Actually giving people a $25 voucher would likely be more effective at upping the vaccination rates and money a good deal better spent than millions on any other form of advertising and propaganda