 Please don’t have to bring out your dead.
Please don’t have to bring out your dead.
Written By:
- Date published:
12:27 pm, March 29th, 2020 - 45 comments
Categories: covid-19, Economy, health, Social issues, tourism, uncategorized -
Tags: epidemic, future, pandemic
Anyone who has read even briefly into written human history is going to be aware that it is as much defined by our epidemics and pandemics as by any of our technical and societal achievements. This post is essentially a quick range over the history of pandemics and epidemics with links and some focus on COVID-19.
The effects of pandemics is apparent in the written accounts of the Plague of Justinian which winnowed the Eurasia and Africa for from the 6th century and variations repeating to the early 20th century Or the undocumented plagues that repeatedly decimated or destroyed civilisations in the Americas prior to European invasions. Or the plague disasters that followed the colonial empires spreading regional diseases on a grand scale keep reverberating in indigenous populations to the present day.
Most of the diseases that have been common through human history have had their impacts constrained with the awareness of the sources of epidemic diseases, the introduction of better sanitation, the long slow history of developing vaccines, and effective preventative medical treatments.
But through the 20th century, at least in developed world, the ever-present dread and awareness of epidemics that was still residual during my childhood in the 1960s has dissipated. My grandparents lived in aftermath of the 1918 influenza pandemic. My parents grew up as the polio epidemic was attacking their classmates. During my childhood there were continuous mini-epidemics of various infectious diseases from mumps to measles.
Our generations saw the effect of the introductions of vaccines and the loss of knowledge about epidemics in our society diminished.
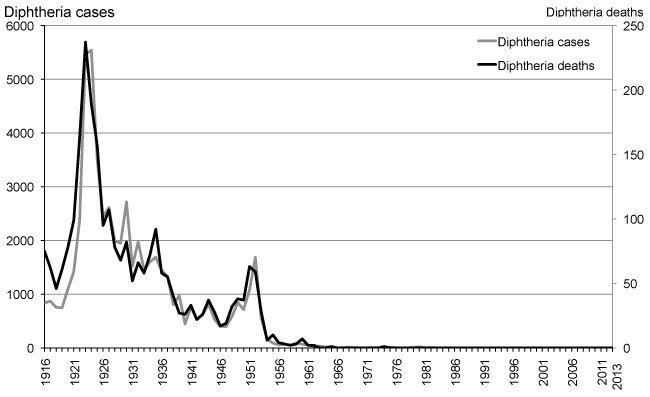
As an example in my life, diphtheria was a disease that well known to my grandparents and parents. But it was disease that I had no idea about. The vaccine was introduced into NZ in 1941 for children under 7 well after the 1921 epidemic. This graph from a 2016 post by Helen Petousis-Harris at Te Pūnaha Matatini “If only there had been a vaccine” displays clearly why I wasn’t aware of it – I was born in 1959.
When I’ve talked to my younger relatives and colleagues, their ignorance of the dangers of diseases that were worried the hell out of my parents when I was growing up is just scary as hell. They simply don’t feel the fragility of the clean water systems that we depend on to stave of outbreaks of diseases like cholera, or why using antibiotics blithely for viral diseases or milk production is a stupid idea, or why using vaccines isn’t an individual choice like what brand of cellphone you like.
This ignorance has been particularly apparent to anyone who has spent time online looking aghast at the deliberate spreading of misinformation by anti-vaxxers over the last decade. Instead of the ever-present dangers of re-emerging diseases, recent generations seem to be more invested in the fantasies of the zombie apocalypse rather than the more mundane concerns about rubella or measles.
Virtually all of the epidemics that have a potential of flaring into pandemics now appear to be emerging infectious diseases especially those noted as being ‘novel’ or previously unknown to our medical histories.
Emerging infectious diseases are infections that have recently appeared within a population or those whose incidence or geographic range is rapidly increasing or threatens to increase in the near future. Emerging infections can be caused by:
- Previously undetected or unknown infectious agents
- Known agents that have spread to new geographic locations or new populations
- Previously known agents whose role in specific diseases has previously gone unrecognized.
- Re-emergence of agents whose incidence of disease had significantly declined in the past, but whose incidence of disease has reappeared. This class of diseases is known as re-emerging infectious diseases.
The World Health Organization warned in its 2007 report that infectious diseases are emerging at a rate that has not been seen before. Since the 1970s, about 40 infectious diseases have been discovered, including SARS, MERS, Ebola, chikungunya, avian flu, swine flu and, most recently, Zika.
With people traveling much more frequently and far greater distances than in the past, living in more densely populated areas, and coming into closer contact with wild animals, the potential for emerging infectious diseases to spread rapidly and cause global epidemics is a major concern.
To that list, we can now add severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) – the virus strain that causes COVID-19. This is probably a well established viral disease in bat populations that has recently made the jump to humans via an immediate species.
Inter-species crossover has been a common theme in novel infectious diseases. HIV probably crossed over from chimpanzees in the early 20th century. MERS is probably a crossover from camels. Ebola probably also from bats via infected apes. Avian flus mostly from from birds and swine flu mostly from pigs as their names indicate.
The issue with novel diseases is that when they do managed to have an inter-species crossover that allows for a successful intra-species infection in humans, they are sometimes extremely infectious. Frequently they’re so infectious that they are self-limiting.
Ebola is like this. When it gets into a susceptible population with poor medical support with social hygiene and customs that facilitate immediate transmission, the outbreaks burn themselves out fast. That is because the association between caring for patients or grieving for the dead becomes obvious within a short period to survivors.
This is a self-limiting strategy for the disease. To date Ebola has had limited success infecting anyone outside of central Africa despite a number of infected travellers, particularly in 2014.
The 2003 SARS outbreak was contained primarily because the number of people with mild symptoms were low. It also did not have a . This made isolation of the infected, the containment and testing of people that were associated with, and the eventual eradication of the disease feasible. But there was also a healthy dose of just luck as a World Health Organisation after-action-review made clear:-
The rapid containment of SARS is a success in public health, but also a warning. It is proof of the power of international collaboration supported at the highest political level. It is also proof of the effectiveness of GOARN in detecting and responding to emerging infections of international public health importance. At the same time, containment of SARS was aided by good fortune. The most severely affected areas in the SARS outbreak had well-developed health care systems. Had SARS established a foothold in countries where health systems are less well developed cases might still be occurring, with global containment much more difficult, if not impossible.
Although control measures were effective, they were extremely disruptive and consumed enormous resources — resources that might not have been sustainable over time. If SARS reoccurs during an influenza season, health systems worldwide will be put under extreme pressure as they seek to isolate all those who fit the clinical case definition until diagnosis can be ascertained. Continued vigilance is vital.
This chapter has illustrated how quickly a new disease can threaten global health. Thankfully, not all diseases move at such speed; but some are more stealthy and more lethal.
The SARS epidemic was contained within 12 months. Which in retrospect was somewhat unfortunate. Most of the advanced efforts to get an effective vaccine or treatment against SARS were shelved as the epidemic was being contained or in the decade following in a classic case of failing to be actively proactive after a scare.
There are a number of vaccines that were developed. Many of which had issues with the effect of the vaccine causing over-energetic responses in test subject’s auto-immune systems and increased symptoms. Unfortunately excessive auto-immune responses are also the main cause of fatalities with both SARS and COVID-19.
The COVID-19 is in many ways similar with the 2003 SARS outbreak as this Lancet article “Can we contain the COVID-19 outbreak with the same measures as for SARS?” but has some differences that make it far more stealthy.
Clear differences are emerging, such as in transmissibility and severity pyramids; COVID-19 has a higher transmissibility than SARS, and many more patients with COVID-19 rather than SARS have mild symptoms that contribute to spread because these patients are often missed and not isolated.
Mild symptoms with COVID-19 are really really problematic for containment because of the viral shedding as this quotation from the Lancet article makes clear (my italics).
Isolation was effective for SARS because peak viral shedding occurred after patients were already quite ill with respiratory symptoms and could be easily identified. Although asymptomatic or mildly symptomatic patients have been reported for SARS,35 no known transmission occurred from these patients. By contrast, preliminary evidence from exported COVID-19 cases suggest that transmission during the early phase of illness also seems to contribute to overall transmission;36, 37 therefore, isolation of more severely ill patients at the time of presentation to health-care facilities will be too late. The effectiveness of isolation and contact tracing methods depends on the proportion of transmission that occurs before symptom onset. Pre-symptomatic transmission will also make temperature screening less effective.38
In other words, with COVID-19 you can be infected with few or even no symptoms and still infect others as a carrier. With SARS it could be contained because people who had it were symptomatic and infectious or non-symptomatic and apparently not infectious. What is also known is that people who have gotten over the disease can also shed viruses for some time afterwards. The European CDC says in their discharge criteria
SARS-CoV-2 virus can initially be detected 1–2 days prior to symptom onset in upper respiratory tract samples; the virus can persist for 7–12 days in moderate cases and up to 2 weeks in severe cases (WHO mission to China Report) [1]. In faeces, viral RNA has been detected in up to 30% of patients from day 5 after onset and up to 4 to 5 weeks in moderate cases. The significance of faecal viral shedding for transmission still has to be clarified [1].
In the absence of a vaccine or preventative treatment, the mild symptomatic infection and potentially long shedding periods mean in most places containment is likely to fail as strategy.
While potential for fast report antibody tests will capable of detecting if someone has contacted the disease. However as the New Scientist and others pointed out
If we know someone has had the virus, they can potentially leave their home without risk of being re-infected, which would help countries get moving again. However, the accuracy of the tests has yet to be established. “The one thing that’s worse than no test is an inaccurate test,” Chris Whitty, the UK’s chief medical adviser, said on 25 March. Someone wrongly told they have already had covid-19 could go out and get infected.
and
The antibody response to the coronavirus may be delayed compared with other infections. The tests can be used only 14 days or more after people develop symptoms, says Adams.
This also means antibody testing will be of limited use for tracing the contacts of infected people – which many think is crucial for controlling the outbreak – because health authorities will be weeks behind.
Plus a positive antibody test doesn’t indicate where people are in the virus shedding cycle. Currently only a swab test taken by trained personnel and sent to lab for analysis will do that.
Which makes Boris Johnson’s enthusiasm for the antibody test (even assuming it works as advertised) as being ‘game-changer’ ridiculous. It serves more as an indication of his habit of being a dangerously ignorant idiot. The New Scientist article ends with a better informed and thought through analysis..
On the plus side, many groups are working on faster genetic tests and on antigen tests that can detect the virus in, say, saliva. Testing widely for both active infections and past infections should be a highly effective combination.
Of course to make that work for getting people back into the workforce, we’d probably need to bulk-order bracelets to allow confirmation for people who can be out and about because they neither get nor infect with the virus. I’d imagine that in NZ that being required to carry infection status identity will, in itself, cause some debate.
However in New Zealand we have what Jacinda Ardern describes as a “reasonable” chance of doing a containment strategy. Closed borders apart from those kiwis and their spouses and dependents still able to make it back, a slowly increasingly strict isolation policy for arrivals, and a lock-down for 4 weeks make it possible.
My background as a part-time army medic and as a lifelong student of the history of epidemics makes me want to get somewhat draconian.
For travellers arriving, our continuing primary disease vector, we should use the isolation model that Taiwan has been using. Ensure that people in isolation have food delivered and don’t have to leave. If they are in a hotel or home then require active tracking the GPS of phones, and regularly and randomly auto-poll that phone to make sure that the owner is next to the phone. One article I read on Medium which I can’t find now described the wakeup call that one taiwanese arrival got when their cellphone battery ran out of power and they had police banging on their door shortly afterwards.
If people don’t follow the common sense rules for isolation to prevent the spread of infection, then I’m sure that we can find an island and a tent to drop them on for a month until the court has time to deal with them. At the very least it will prevent them to be being a stupid danger to others.
I’d suggest that the same happens to the owner or manager of businesses who self-deem themselves to be ‘essential’. Not only are they putting customers in danger, but presumably they’re also pressuring employees to do it as well.
The biggest problems for NZ with our current strategy is to prevent issues with community transfer during and after the release of the lockdown. This would result in lockdowns extending or resuming in areas – often far wider than local areas.
So far I’m not optimistic that a single national lockdown will be completely effective because people seem to be taking some very liberal interpretations of what a household ‘bubble’ means. There are anecdotal reports of household bubbles joining up so that their kids can play together. Or kids playing games in parks. Its going to be interesting see how this plays out in the coming weeks. Each of these effectively widen out any lockdown to quarantine outbreaks.
Hopefully someone has started to do location tracking on cellphones to find out what are actual ‘local’ areas as evidenced by actual aggregate movements.
If our containment strategy does work and community spread is eliminated. Then the big question is – how we reconnect to rest of the world?
We’d wind up with a small number of immune people and most people being susceptible. At the very least, we’d need to have border antibody and live virus tests before people boarded and a rapid retest on arrival. Validation of the error rates on combinations of tests will determine the risk levels. Otherwise tourists, business travel, and returning kiwis will require 14 days quarantine.
Our tourist industry will be hanging out for a vaccine in NZ. Realistically before we can start up Hobbiton we’d require a largely immune population.
As importantly, before we restart our tourism industry or to allow kiwis to fly offshore again, we’re going to need to have a very close look at how we deal with the next ‘novel’ disease. I, for one, have absolutely no real interest in dying for tourism.
Basically we are trying to do with our containment strategies is to avoid the modern analogue in a covid-19 Italy and elsewhere of “bring out your dead”. This was the defining civic characteristic of past pandemics.
In Italy, as the fatalities of covid-19 overwhelm the funeral systems we get the military being called in to transport the dead.
Italian army called in to help transport the dead – REUTERS
At least it is a bit more civilised and dignified than the black humour of Monty Python’s depiction of the same task in a medieval plague.
Anything is better than that.
45 comments on “Please don’t have to bring out your dead. ”
- Comments are now closed
- Comments are now closed
Recent Comments
- 2024 SkS Weekly Climate Change & Global Warming News Roundup #51
 A listing of 25 news and opinion articles we found interesting and shared on social media during the past week: Sun, December 15, 2024 thru Sat, December 21, 2024. Based on feedback we received, this week's roundup is the first one published soleley by category. We are still interested in ...1 hour ago
A listing of 25 news and opinion articles we found interesting and shared on social media during the past week: Sun, December 15, 2024 thru Sat, December 21, 2024. Based on feedback we received, this week's roundup is the first one published soleley by category. We are still interested in ...1 hour ago - Dance Magic
 Well, I've been there, sitting in that same chairWhispering that same prayer half a million timesIt's a lie, though buried in disciplesOne page of the Bible isn't worth a lifeThere's nothing wrong with youIt's true, it's trueThere's something wrong with the villageWith the villageSomething wrong with the villageSongwriters: Andrew Jackson ...13 hours ago
Well, I've been there, sitting in that same chairWhispering that same prayer half a million timesIt's a lie, though buried in disciplesOne page of the Bible isn't worth a lifeThere's nothing wrong with youIt's true, it's trueThere's something wrong with the villageWith the villageSomething wrong with the villageSongwriters: Andrew Jackson ...13 hours ago - Government Forces Universities to Enforce “Free Speech” While Limiting Universities̵...
 ACT would like to dictate what universities can and can’t say. We knew it was coming. It was outlined in the coalition agreement and has become part of Seymour’s strategy of “emphasising public funding” to prevent people from opposing him and his views—something he also uses to try and de-platform ...13 hours ago
ACT would like to dictate what universities can and can’t say. We knew it was coming. It was outlined in the coalition agreement and has become part of Seymour’s strategy of “emphasising public funding” to prevent people from opposing him and his views—something he also uses to try and de-platform ...13 hours ago - Fact brief – Are we heading into an ‘ice age’?
Skeptical Science is partnering with Gigafact to produce fact briefs — bite-sized fact checks of trending claims. This fact brief was written by Sue Bin Park from the Gigafact team in collaboration with members from our team. You can submit claims you think need checking via the tipline. Are we heading ...1 day ago
- As Our Power Lessens: Published
 So the Solstice has arrived – Summer in this part of the world, Winter for the Northern Hemisphere. And with it, the publication my new Norse dark-fantasy piece, As Our Power Lessens at Eternal Haunted Summer: https://eternalhauntedsummer.com/issues/winter-solstice-2024/as-our-power-lessens/ As previously noted, this one is very ‘wyrd’, and Northern Theory of Courage. ...1 day ago
So the Solstice has arrived – Summer in this part of the world, Winter for the Northern Hemisphere. And with it, the publication my new Norse dark-fantasy piece, As Our Power Lessens at Eternal Haunted Summer: https://eternalhauntedsummer.com/issues/winter-solstice-2024/as-our-power-lessens/ As previously noted, this one is very ‘wyrd’, and Northern Theory of Courage. ...1 day ago - By Any Other Name.
 The Natural Choice: As a starter for ten percent of the Party Vote, “saving the planet” is a very respectable objective. Young voters, in particular, raised on the dire (if unheeded) warnings of climate scientists, and the irrefutable evidence of devastating weather events linked to global warming, vote Green. After ...1 day ago
The Natural Choice: As a starter for ten percent of the Party Vote, “saving the planet” is a very respectable objective. Young voters, in particular, raised on the dire (if unheeded) warnings of climate scientists, and the irrefutable evidence of devastating weather events linked to global warming, vote Green. After ...1 day ago - Bernard’s last Saturday Soliloquy for 2024
 The Government cancelled 60% of Kāinga Ora’s new builds next year, even though the land for them was already bought, the consents were consented and there are builders unemployed all over the place. Photo: Lynn Grieveson / The KākāMōrena. Long stories short, the six things that mattered in Aotearoa’s political ...2 days ago
The Government cancelled 60% of Kāinga Ora’s new builds next year, even though the land for them was already bought, the consents were consented and there are builders unemployed all over the place. Photo: Lynn Grieveson / The KākāMōrena. Long stories short, the six things that mattered in Aotearoa’s political ...2 days ago - Bernard’s Picks ‘n’ Mixes for Saturday, December 21
 Photo by CHUTTERSNAP on UnsplashEvery morning I get up at 3am to go around the traps of news sites in Aotearoa and globally. I pick out the top ones from my point of view and have been putting them into my Dawn Chorus email, which goes out with a podcast. ...2 days ago
Photo by CHUTTERSNAP on UnsplashEvery morning I get up at 3am to go around the traps of news sites in Aotearoa and globally. I pick out the top ones from my point of view and have been putting them into my Dawn Chorus email, which goes out with a podcast. ...2 days ago - 2024 OIA stats
 Over on Kikorangi Newsroom's Marc Daalder has published his annual OIA stats. So I thought I'd do mine: 82 OIA requests sent in 2024 7 posts based on those requests 20 average working days to receive a response Ministry of Justice was my most-requested entity, ...2 days ago
Over on Kikorangi Newsroom's Marc Daalder has published his annual OIA stats. So I thought I'd do mine: 82 OIA requests sent in 2024 7 posts based on those requests 20 average working days to receive a response Ministry of Justice was my most-requested entity, ...2 days ago - Climate Change: A perverse incentive
The government published its first Biennial Transparency Report under the Paris Agreement yesterday, and the media has correctly noted that it is missing any plan to actually meet our target. While it hypes domestic emissions reductions so far - which have been good, but will likely get worse thanks to ...2 days ago
- Economic Bulletin December 2024
 Welcome to the December 2024 Economic Bulletin. We have two monthly features in this edition. In the first, we discuss what the Half Year Economic and Fiscal Update from Treasury and the Budget Policy Statement from the Minister of Finance tell us about the fiscal position and what to ...2 days ago
Welcome to the December 2024 Economic Bulletin. We have two monthly features in this edition. In the first, we discuss what the Half Year Economic and Fiscal Update from Treasury and the Budget Policy Statement from the Minister of Finance tell us about the fiscal position and what to ...2 days ago - NZCTU make submission in opposition to Treaty Principles Bill
The NZCTU Te Kauae Kaimahi have submitted against the controversial Treaty Principles Bill, slamming the Bill as a breach of Te Tiriti o Waitangi and an attack on tino rangatiratanga and the collective rights of Tangata Whenua. “This Bill seeks to legislate for Te Tiriti o Waitangi principles that are ...2 days ago
- ZB’s Power Couple
 I don't knowHow to say what's got to be saidI don't know if it's black or whiteThere's others see it redI don't get the answers rightI'll leave that to youIs this love out of fashionOr is it the time of yearAre these words distraction?To the words you want to hearSongwriters: ...3 days ago
I don't knowHow to say what's got to be saidI don't know if it's black or whiteThere's others see it redI don't get the answers rightI'll leave that to youIs this love out of fashionOr is it the time of yearAre these words distraction?To the words you want to hearSongwriters: ...3 days ago - Austerity thumps GDP most since 1991
Our economy has experienced its worst recession since 1991. Photo: Lynn Grieveson / The KākāMōrena. Long stories short, the six things that matter in Aotearoa’s political economy around housing, climate and poverty on Friday, December 20 in The Kākā’s Dawn Chorus podcast above and the daily Pick ‘n’ Mix below ...3 days ago
- Weekly Roundup 20-December-2024
 Twas the Friday before Christmas and all through the week we’ve been collecting stories for our final roundup of the year. As we start to wind down for the year we hope you all have a safe and happy Christmas and new year. If you’re travelling please be safe on ...3 days ago
Twas the Friday before Christmas and all through the week we’ve been collecting stories for our final roundup of the year. As we start to wind down for the year we hope you all have a safe and happy Christmas and new year. If you’re travelling please be safe on ...3 days ago - The Hoon around the year to December 20, 2024
The podcast above of the weekly ‘Hoon’ webinar for paying subscribers on Thursday night features co-hosts & talking about the year’s news with: on climate. Her book of the year was Tim Winton’s cli-fi novel Juice and she also mentioned Mike Joy’s memoir The Fight for Fresh Water. ...3 days ago
- The baby-boomers’ last gasp
 The Government can head off to the holidays, entitled to assure itself that it has done more or less what it said it would do. The campaign last year promised to “get New Zealand back on track.” When you look at the basic promises—to trim back Government expenditure, toughen up ...3 days ago
The Government can head off to the holidays, entitled to assure itself that it has done more or less what it said it would do. The campaign last year promised to “get New Zealand back on track.” When you look at the basic promises—to trim back Government expenditure, toughen up ...3 days ago - Skeptical Science New Research for Week #51 2024
Open access notables An intensification of surface Earth’s energy imbalance since the late 20th century, Li et al., Communications Earth & Environment: Tracking the energy balance of the Earth system is a key method for studying the contribution of human activities to climate change. However, accurately estimating the surface energy balance ...3 days ago
- Join us at 5pm for 2024’s last Hoon
 Photo by Mauricio Fanfa on UnsplashKia oraCome and join us for our weekly ‘Hoon’ webinar with paying subscribers to The Kākā for an hour at 5 pm today.Jump on this link on YouTube Livestream for our chat about the week’s news with myself , plus regular guests and , ...3 days ago
Photo by Mauricio Fanfa on UnsplashKia oraCome and join us for our weekly ‘Hoon’ webinar with paying subscribers to The Kākā for an hour at 5 pm today.Jump on this link on YouTube Livestream for our chat about the week’s news with myself , plus regular guests and , ...3 days ago - Christmas Gifts: Ageing Boomers, Laurie & Les, Talk Politics.
“Like you said, I’m an unreconstructed socialist. Everybody deserves to get something for Christmas.”“ONE OF THOSE had better be for me!” Hannah grinned, fascinated, as Laurie made his way, gingerly, to the bar, his arms full of gift-wrapped packages.“Of course!”, beamed Laurie. Depositing his armful on the bar-top and selecting ...3 days ago
- GDP Figures No Christmas Present for New Zealand
Data released by Statistics New Zealand today showed a significant slowdown in the economy over the past six months, with GDP falling by 1% in September, and 1.1% in June said CTU Economist Craig Renney. “The data shows that the size of the economy in GDP terms is now smaller ...3 days ago
- Cheeseburgers and Stunt Monkeys
 One last thing before I quitI never wanted any moreThan I could fit into my headI still remember every single word you saidAnd all the shit that somehow came along with itStill, there's one thing that comforts meSince I was always caged and now I'm freeSongwriters: David Grohl / Georg ...3 days ago
One last thing before I quitI never wanted any moreThan I could fit into my headI still remember every single word you saidAnd all the shit that somehow came along with itStill, there's one thing that comforts meSince I was always caged and now I'm freeSongwriters: David Grohl / Georg ...3 days ago - MSD rejecting 220 pleas for food grants each day
Sparse offerings outside a Te Kauwhata church. Meanwhile, the Government is cutting spending in ways that make thousands of hungry children even hungrier, while also cutting funding for the charities that help them. It’s also doing that while winding back new building of affordable housing that would allow parents to ...4 days ago
- The Wing Parties’ Economic Policies.
 It is difficult to make sense of the Luxon Coalition Government’s economic management.This end-of-year review about the state of economic management – the state of the economy was last week – is not going to cover the National Party contribution. Frankly, like every other careful observer, I cannot make up ...4 days ago
It is difficult to make sense of the Luxon Coalition Government’s economic management.This end-of-year review about the state of economic management – the state of the economy was last week – is not going to cover the National Party contribution. Frankly, like every other careful observer, I cannot make up ...4 days ago - Back on Track
 This morning I awoke to the lovely news that we are firmly back on track, that is if the scale was reversed.NZ ranks low in global economic comparisonsNew Zealand's economy has been ranked 33rd out of 37 in an international comparison of which have done best in 2024.Economies were ranked ...4 days ago
This morning I awoke to the lovely news that we are firmly back on track, that is if the scale was reversed.NZ ranks low in global economic comparisonsNew Zealand's economy has been ranked 33rd out of 37 in an international comparison of which have done best in 2024.Economies were ranked ...4 days ago - Book Review: How Big Things Get Done
This is a guest post by George Weeks, reviewing a book called How Big Things Get Done by Bent Flyvbjerg and Dan Gardner Want to know how to do something big? Ask someone who has done it before! Professor Bent Flyvbjerg has spent his career studying megaprojects. In 2023, ...4 days ago
- Gordon Campbell On Why We Can’t Survive Two More Years Of This
 Remember those silent movies where the heroine is tied to the railway tracks or going over the waterfall in a barrel? Finance Minister Nicola Willis seems intent on portraying herself as that damsel in distress. According to Willis, this country’s current economic problems have all been caused by the spending ...4 days ago
Remember those silent movies where the heroine is tied to the railway tracks or going over the waterfall in a barrel? Finance Minister Nicola Willis seems intent on portraying herself as that damsel in distress. According to Willis, this country’s current economic problems have all been caused by the spending ...4 days ago - Dragging our way towards the finish line, the end of this year can’t come soon enough for many…
 Similar to the cuts and the austerity drive imposed by Ruth Richardson in the 1990’s, an era which to all intents and purposes we’ve largely fiddled around the edges with fixing in the time since – over, to be fair, several administrations – whilst trying our best it seems to ...4 days ago
Similar to the cuts and the austerity drive imposed by Ruth Richardson in the 1990’s, an era which to all intents and purposes we’ve largely fiddled around the edges with fixing in the time since – over, to be fair, several administrations – whilst trying our best it seems to ...4 days ago - Handling Democracy.
String-Pulling in the Dark: For the democratic process to be meaningful it must also be public. WITH TRUST AND CONFIDENCE in New Zealand’s politicians and journalists steadily declining, restoring those virtues poses a daunting challenge. Just how daunting is made clear by comparing the way politicians and journalists treated New Zealanders ...4 days ago
- Open letter to the Minister of Dwindling Finances
 Dear Nicola Willis, thank you for letting us know in so many words that the swingeing austerity hasn't worked.By in so many words I mean the bit where you said, Here is a sea of red ink in which we are drowning after twelve months of savage cost cutting and ...4 days ago
Dear Nicola Willis, thank you for letting us know in so many words that the swingeing austerity hasn't worked.By in so many words I mean the bit where you said, Here is a sea of red ink in which we are drowning after twelve months of savage cost cutting and ...4 days ago - Open Government: The joke ends
The Open Government Partnership is a multilateral organisation committed to advancing open government. Countries which join are supposed to co-create regular action plans with civil society, committing to making verifiable improvements in transparency, accountability, participation, or technology and innovation for the above. And they're held to account through an Independent ...4 days ago
- An unusual sort of press conference
 Today I tuned into something strange: a press conference that didn’t make my stomach churn or the hairs on the back of my neck stand on end. Which was strange, because it was about the torture of children. It was the announcement by Erica Stanford — on her own, unusually ...4 days ago
Today I tuned into something strange: a press conference that didn’t make my stomach churn or the hairs on the back of my neck stand on end. Which was strange, because it was about the torture of children. It was the announcement by Erica Stanford — on her own, unusually ...4 days ago - This substack has talked about this government’s seeming corruption & pro-corporate issues...
 This is a must watch, and puts on brilliant and practical display the implications and mechanics of fast-track law corruption and weakness.CLICK HERE: LINK TO WATCH VIDEOOur news media as it is set up is simply not equipped to deal with the brazen disinformation and corruption under this right wing ...4 days ago
This is a must watch, and puts on brilliant and practical display the implications and mechanics of fast-track law corruption and weakness.CLICK HERE: LINK TO WATCH VIDEOOur news media as it is set up is simply not equipped to deal with the brazen disinformation and corruption under this right wing ...4 days ago - NZCTU: Minister needs to listen to the evidence on engineered stone ban
NZCTU Te Kauae Kaimahi Acting Secretary Erin Polaczuk is welcoming the announcement from Minister of Workplace Relations and Safety Brooke van Velden that she is opening consultation on engineered stone and is calling on her to listen to the evidence and implement a total ban of the product. “We need ...4 days ago
- Wednesday 18 December
The Government has announced a 1.5% increase in the minimum wage from 1 April 2025, well below forecast inflation of 2.5%. Unions have reacted strongly and denounced it as a real terms cut. PSA and the CTU are opposing a new round of staff cuts at WorkSafe, which they say ...4 days ago
- Can the government change its mind on the ferries?
The decision to unilaterally repudiate the contract for new Cook Strait ferries is beginning to look like one of the stupidest decisions a New Zealand government ever made. While cancelling the ferries and their associated port infrastructure may have made this year's books look good, it means higher costs later, ...4 days ago
- Notes from Afar: Will Luxon Attend Waitangi Day? And Opposition Calls Out Nicola Willis for “C...
 Hi there! I’ve been overseas recently, looking after a situation with a family member. So apologies if there any less than focused posts! Vanuatu has just had a significant 7.3 earthquake. Two MFAT staff are unaccounted for with local fatalities.It’s always sad to hear of such things happening.I think of ...5 days ago
Hi there! I’ve been overseas recently, looking after a situation with a family member. So apologies if there any less than focused posts! Vanuatu has just had a significant 7.3 earthquake. Two MFAT staff are unaccounted for with local fatalities.It’s always sad to hear of such things happening.I think of ...5 days ago - Member’s morning
Today is a special member's morning, scheduled to make up for the government's theft of member's days throughout the year. First up was the first reading of Greg Fleming's Crimes (Increased Penalties for Slavery Offences) Amendment Bill, which was passed unanimously. Currently the House is debating the third reading of ...5 days ago
- Going Backwards
 We're going backwardsIgnoring the realitiesGoing backwardsAre you counting all the casualties?We are not there yetWhere we need to beWe are still in debtTo our insanitiesSongwriter: Martin Gore Read more ...5 days ago
We're going backwardsIgnoring the realitiesGoing backwardsAre you counting all the casualties?We are not there yetWhere we need to beWe are still in debtTo our insanitiesSongwriter: Martin Gore Read more ...5 days ago - Blaming Treasury & Labour, Willis looks for even more Austerity
Willis blamed Treasury for changing its productivity assumptions and Labour’s spending increases since Covid for the worsening Budget outlook. Photo: Getty ImagesMōrena. Long stories short, the six things that matter in Aotearoa’s political economy around housing, climate and poverty on Wednesday, December 18 in The Kākā’s Dawn Chorus podcast above ...5 days ago
- December-24 AT Board Meeting
Today the Auckland Transport board meet for the last time this year. For those interested (and with time to spare), you can follow along via this MS Teams link from 10am. I’ve taken a quick look through the agenda items to see what I think the most interesting aspects are. ...5 days ago
- The Making of a Mental Health Rockstar
 Hi,If you’re a New Zealander — you know who Mike King is. He is the face of New Zealand’s battle against mental health problems. He can be loud and brash. He raises, and is entrusted with, a lot of cash. Last year his “I Am Hope” charity reported a revenue ...5 days ago
Hi,If you’re a New Zealander — you know who Mike King is. He is the face of New Zealand’s battle against mental health problems. He can be loud and brash. He raises, and is entrusted with, a lot of cash. Last year his “I Am Hope” charity reported a revenue ...5 days ago - It could have been worse
Probably about the only consolation available from yesterday’s unveiling of the Half-Yearly Economic and Fiscal Update (HYEFU) is that it could have been worse. Though Finance Minister Nicola Willis has tightened the screws on future government spending, she has resisted the calls from hard-line academics, fiscal purists and fiscal hawks ...5 days ago
- The Deep Divisions of Local Government
 The right have a stupid saying that is only occasionally true:When is democracy not democracy? When it hasn’t been voted on.While not true in regards to branches of government such as the judiciary, it’s a philosophy that probably should apply to recently-elected local government councillors. Nevertheless, this concept seemed to ...5 days ago
The right have a stupid saying that is only occasionally true:When is democracy not democracy? When it hasn’t been voted on.While not true in regards to branches of government such as the judiciary, it’s a philosophy that probably should apply to recently-elected local government councillors. Nevertheless, this concept seemed to ...5 days ago - Willis’ austerity strategy just isn’t working
Long story short: the Government’s austerity policy has driven the economy into a deeper and longer recession that means it will have to borrow $20 billion more over the next four years than it expected just six months ago. Treasury’s latest forecasts show the National-ACT-NZ First Government’s fiscal strategy of ...5 days ago
- Sabin 33 #7 – Are solar projects hurting farmers and rural communities?
On November 1, 2024 we announced the publication of 33 rebuttals based on the report "Rebutting 33 False Claims About Solar, Wind, and Electric Vehicles" written by Matthew Eisenson, Jacob Elkin, Andy Fitch, Matthew Ard, Kaya Sittinger & Samuel Lavine and published by the Sabin Center for Climate Change Law at Columbia ...5 days ago
- Join us for a pop-up Hoon at 5pm on HYEFU
 5 days ago
5 days ago - ‘Ideas Worth Saving’: A Call for Papers
 Some years ago, I found myself pondering the power of literature to endure. Or at least the power of some of it to endure, while the rest vanishes in mere decades: https://phuulishfellow.wordpress.com/2019/08/07/look-on-my-works-ye-mighty-and-despair-the-literary-future/. I have similarly had fun with the subject in some of my short stories, such as Another Alexandria ...5 days ago
Some years ago, I found myself pondering the power of literature to endure. Or at least the power of some of it to endure, while the rest vanishes in mere decades: https://phuulishfellow.wordpress.com/2019/08/07/look-on-my-works-ye-mighty-and-despair-the-literary-future/. I have similarly had fun with the subject in some of my short stories, such as Another Alexandria ...5 days ago - Corrections is torturing prisoners again
In 1998, in the wake of the Paremoremo Prison riot, the Department of Corrections established the "Behaviour Management Regime". Prisoners were locked in their cells for 22 or 23 hours a day, with no fresh air, no exercise, no social contact, no entertainment, and in some cases no clothes and ...5 days ago
- HYEFU and BPS data shows New Zealand is way off track
New data released by the Treasury shows that the economic policies of this Government have made things worse in the year since they took office, said NZCTU Economist Craig Renney. “Our fiscal indicators are all heading in the wrong direction – with higher levels of debt, a higher deficit, and ...5 days ago
- “Better economic management”
At the 2023 election, National basically ran on a platform of being better economic managers. So how'd that turn out for us? In just one year, they've fucked us for two full political terms: The government's books are set to remain deeply in the red for the near term ...5 days ago
- Shameless, clueless
 AUSTERITYText within this block will maintain its original spacing when publishedMy spreadsheet insists This pain leads straight to glory (File not found) Read more ...5 days ago
AUSTERITYText within this block will maintain its original spacing when publishedMy spreadsheet insists This pain leads straight to glory (File not found) Read more ...5 days ago - Minimum wage ‘increase’ is an effective cut
The NZCTU Te Kauae Kaimahi are saying that the Government should do the right thing and deliver minimum wage increases that don’t see workers fall further behind, in response to today’s announcement that the minimum wage will only be increased by 1.5%, well short of forecast inflation. “With inflation forecast ...5 days ago
- Crazy ’bout a Sharp-dressed Man
 Oh, I weptFor daysFilled my eyesWith silly tearsOh, yeaBut I don'tCare no moreI don't care ifMy eyes get soreSongwriters: Paul Rodgers / Paul Kossoff. Read more ...6 days ago
Oh, I weptFor daysFilled my eyesWith silly tearsOh, yeaBut I don'tCare no moreI don't care ifMy eyes get soreSongwriters: Paul Rodgers / Paul Kossoff. Read more ...6 days ago - How much should you worry about a collapse of the Atlantic conveyor belt?
This is a re-post from Yale Climate Connections by Bob Henson In this aerial view, fingers of meltwater flow from the melting Isunnguata Sermia glacier descending from the Greenland Ice Sheet on July 11, 2024, near Kangerlussuaq, Greenland. According to the Programme for Monitoring of the Greenland Ice Sheet (PROMICE), the ...6 days ago
- 8% ACT Party Creates One Ring To Rule Them All
 In August, I wrote an article about David Seymour1 with a video of his testimony, to warn that there were grave dangers to his Ministry of Regulation:David Seymour's Ministry of Slush Hides Far Greater RisksWhy Seymour's exorbitant waste of taxpayers' money could be the least of concernThe money for Seymour ...6 days ago
In August, I wrote an article about David Seymour1 with a video of his testimony, to warn that there were grave dangers to his Ministry of Regulation:David Seymour's Ministry of Slush Hides Far Greater RisksWhy Seymour's exorbitant waste of taxpayers' money could be the least of concernThe money for Seymour ...6 days ago - When austerity worsens public debt & cuts GDP
Willis is expected to have to reveal the bitter fiscal fruits of her austerity strategy in the HYEFU later today. Photo: Lynn Grieveson/TheKakaMōrena. Long stories short, the six things that matter in Aotearoa’s political economy around housing, climate and poverty on Tuesday, December 17 in The Kākā’s Dawn Chorus podcast ...6 days ago
- Govt to double number of toll roads
On Friday the government announced it would double the number of toll roads in New Zealand as well as make a few other changes to how toll roads are used in the country. The real issue though is not that tolling is being used but the suggestion it will make ...6 days ago
- Luxon’s pre-emptive strike
The Prime Minister yesterday engaged in what looked like a pre-emptive strike designed to counter what is likely to be a series of depressing economic statistics expected before the end of the week. He opened his weekly post-Cabinet press conference with a recitation of the Government’s achievements. “It certainly has ...6 days ago
- Gordon Campbell On The Coalition’s Empty Gestures, And Abortion Refusal As The New Slavery
This whooping cough story from south Auckland is a good example of the coalition government’s approach to social need – spend money on urging people to get vaccinated but only after you’ve cut the funding to where they could get vaccinated. This has been the case all year with public ...6 days ago
- More public service contempt of parliament
Back in 2023 the New Zealand Council for Civil Liberties raised concerns about the inherent conflict of interest involved in public service agencies supporting parliamentary select committees. Our parliament is run on a shoestring, so depends on the public service for advice. But public service agencies work for Ministers, not ...6 days ago
- If There Is A God
 And if there is a GodI know he likes to rockHe likes his loud guitarsHis spiders from MarsAnd if there is a GodI know he's watching meHe likes what he seesBut there's trouble on the breezeSongwriter: William Patrick Corgan Read more ...6 days ago
And if there is a GodI know he likes to rockHe likes his loud guitarsHis spiders from MarsAnd if there is a GodI know he's watching meHe likes what he seesBut there's trouble on the breezeSongwriter: William Patrick Corgan Read more ...6 days ago - A Lipstick Government
 Here’s a quick round up of today’s political news:1. MORE FOOD BANKS, CHARITIES, DOMESTIC VIOLENCE SHELTERS AND YOUTH SOCIAL SERVICES SET TO CLOSE OR SCALE BACK AROUND THE COUNTRY AS GOVT CUTS FUNDINGSome of Auckland's largest foodbanks are warning they may need to close or significantly reduce food parcels after ...6 days ago
Here’s a quick round up of today’s political news:1. MORE FOOD BANKS, CHARITIES, DOMESTIC VIOLENCE SHELTERS AND YOUTH SOCIAL SERVICES SET TO CLOSE OR SCALE BACK AROUND THE COUNTRY AS GOVT CUTS FUNDINGSome of Auckland's largest foodbanks are warning they may need to close or significantly reduce food parcels after ...6 days ago - NZCTU open letter to Treasury on undue restrictions on restricted briefings
Iain Rennie, CNZMSecretary and Chief Executive to the TreasuryDear Secretary, Undue restrictions on restricted briefings This week, the Treasury barred representatives from four organisations, including the New Zealand Council of Trade Unions Te Kauae Kaimahi, from attending the restricted briefing for the Half-Year Economic and Fiscal Update. We had been ...6 days ago
- Why you won’t hear me advocate for electric cars
This is a guest post by Tim Adriaansen, a community, climate, and accessibility advocate. I won’t shut up about climate breakdown, and whenever possible I try to shift the focus of a climate conversation towards solutions. But you’ll almost never hear me give more than a passing nod to ...7 days ago
- Coalition forced to back down on tolling Pahiatua track
A grassroots backlash has forced a backdown from Brown, but he is still eyeing up plenty of tolls for other new roads. And the pressure is on Willis to ramp up the Government’s austerity strategy. Photo: Getty ImagesMōrena. Long stories short, the six things that matter in Aotearoa’s political economy ...7 days ago
- Thank You
 Hi all,I'm pretty overwhelmed by all your messages and emails today; thank you so very much.As much as my newsletter this morning was about money, and we all need to earn money, it was mostly about world domination if I'm honest. 😉I really hate what’s happening to our country, and ...7 days ago
Hi all,I'm pretty overwhelmed by all your messages and emails today; thank you so very much.As much as my newsletter this morning was about money, and we all need to earn money, it was mostly about world domination if I'm honest. 😉I really hate what’s happening to our country, and ...7 days ago - 2024 SkS Weekly Climate Change & Global Warming News Roundup #50
A listing of 23 news and opinion articles we found interesting and shared on social media during the past week: Sun, December 8, 2024 thru Sat, December 14, 2024. Listing by Category Like last week's summary this one contains the list of articles twice: based on categories and based on ...1 week ago
- Making Gravy
 I started writing this morning about Hobson’s Pledge, examining the claims they and their supporters make, basically ripping into them. But I kept getting notifications coming through, and not good ones.Each time I looked up, there was another un-subscription message, and I felt a bit sicker at the thought of ...1 week ago
I started writing this morning about Hobson’s Pledge, examining the claims they and their supporters make, basically ripping into them. But I kept getting notifications coming through, and not good ones.Each time I looked up, there was another un-subscription message, and I felt a bit sicker at the thought of ...1 week ago - Nothing here but the shadows
 Once, long before there was Harry and Meghan and Dodi and all those episodes of The Crown, they came to spend some time with us, Charles and Diana. Was there anyone in the world more glamorous than the Princess of Wales?Dazzled as everyone was by their company, the leader of ...1 week ago
Once, long before there was Harry and Meghan and Dodi and all those episodes of The Crown, they came to spend some time with us, Charles and Diana. Was there anyone in the world more glamorous than the Princess of Wales?Dazzled as everyone was by their company, the leader of ...1 week ago - The United Right: the FSU’s Continued Efforts to Undermine Academia
The collective right have a problem.The entire foundation for their world view is antiscientific. Their preferred economic strategies have been disproven. Their whole neoliberal model faces accusations of corporate corruption and worsening inequality. Climate change not only definitely exists, its rapid progression demands an immediate and expensive response in order ...1 week ago
- Showing the Americans how to do it
Just ten days ago, South Korea's president attempted a self-coup, declaring martial law and attempting to have opposition MPs murdered or arrested in an effort to seize unconstrained power. The attempt was rapidly defeated by the national assembly voting it down and the people flooding the streets to defend democracy. ...1 week ago
- 2 Men, 1 Haircut
 Hi,“What I love about New Zealanders is that sometimes you use these expressions that as Americans we have no idea what those things mean!"I am watching a 30-something year old American ramble on about how different New Zealanders are to Americans. It’s his podcast, and this man is doing a ...1 week ago
Hi,“What I love about New Zealanders is that sometimes you use these expressions that as Americans we have no idea what those things mean!"I am watching a 30-something year old American ramble on about how different New Zealanders are to Americans. It’s his podcast, and this man is doing a ...1 week ago - Chris Penk’s Hate Parade
 What Chris Penk has granted holocaust-denier and equal-opportunity-bigot Candace Owens is not “freedom of speech”. It’s not even really freedom of movement, though that technically is the right she has been granted. What he has given her is permission to perform. Freedom of SpeechIn New Zealand, the right to freedom ...1 week ago
What Chris Penk has granted holocaust-denier and equal-opportunity-bigot Candace Owens is not “freedom of speech”. It’s not even really freedom of movement, though that technically is the right she has been granted. What he has given her is permission to perform. Freedom of SpeechIn New Zealand, the right to freedom ...1 week ago - Tell me a story
 All those tears on your cheeksJust like deja vu flow nowWhen grandmother speaksSo tell me a story (I'll tell you a story)Spell it out, I can't hear (What do you want to hear?)Why you wear black in the morning?Why there's smoke in the air? Songwriter: Greg Johnson.Mōrena all ☀️Something a ...1 week ago
All those tears on your cheeksJust like deja vu flow nowWhen grandmother speaksSo tell me a story (I'll tell you a story)Spell it out, I can't hear (What do you want to hear?)Why you wear black in the morning?Why there's smoke in the air? Songwriter: Greg Johnson.Mōrena all ☀️Something a ...1 week ago
{kind=link}
{kind=link}
{kind=link}
- National’s Greatest Misses 2023-4
 National has only been in power for a year, but everywhere you look, its choices are taking New Zealand a long way backwards. In no particular order, here are the National Government's Top 50 Greatest Misses of its first year in power. ...2 days ago
National has only been in power for a year, but everywhere you look, its choices are taking New Zealand a long way backwards. In no particular order, here are the National Government's Top 50 Greatest Misses of its first year in power. ...2 days ago - Release: Minister’s plan for tertiary sector a backwards step
Returning to the model that was failing for most polytechnics and Institutes of Technology is not the answer. ...2 days ago
- Release: National buries 1019 planned homes
It’s been revealed that National has cancelled 60 percent of its housing projects planned before mid-2025 amidst housing woes. ...3 days ago
- Release: Rule-Czar bill a right-wing power grab
The Government is quietly undertaking consultation on the dangerous Regulatory Standards Bill over the Christmas period to avoid too much attention. ...3 days ago
- Release: Why not both? Luxon shuns Waitangi celebrations
Prime Minister Christopher Luxon is running away from problems of his own creation, with his decision not to go to Waitangi. ...3 days ago
- Govt’s ‘free speech’ legislation stokes fear, not freedom
 The Government’s planned changes to the freedom of speech obligations of universities is little more than a front for stoking the political fires of disinformation and fear, placing teachers and students in the crosshairs. ...3 days ago
The Government’s planned changes to the freedom of speech obligations of universities is little more than a front for stoking the political fires of disinformation and fear, placing teachers and students in the crosshairs. ...3 days ago - Release: Nicola Willis spirals country deeper into recession
The economy shrank 1% this quarter and New Zealand has tumbled into the depths of a recession of Nicola Willis’ making. ...3 days ago
- Release: Hikes for company directors but not ordinary Kiwis
Working people are going backwards while company directors are being given huge pay hikes. ...4 days ago
- ECE no place to cut corners
The Ministry of Regulation’s report into Early Childhood Education (ECE) in Aotearoa raises serious concerns about the possibility of lowering qualification requirements, undermining quality and risking worse outcomes for tamariki, whānau, and kaiako. ...4 days ago
- Release: Strengthening Justice Services for New Zealanders
A Bill to modernise the role of Justices of the Peace (JP), ensuring they remain active in their communities and connected with other JPs, has been put into the ballot. ...4 days ago
- Release: Labour will continue fight against destructive projects
Labour will continue to fight unsustainable and destructive projects that are able to leap-frog environment protection under National’s Fast-track Approvals Bill. ...5 days ago
- Green Government will revoke dodgy fast-track projects
The Green Party has warned that a Green Government will revoke the consents of companies who override environmental protections as part of Fast-Track legislation being passed today. ...5 days ago
- Government for the wealthy keeps pushing austerity
The Green Party says the Half Year Economic and Fiscal Update shows how the Government is failing to address the massive social and infrastructure deficits our country faces. ...5 days ago
- Release: Visa changes let migrant workers be paid less
The Government’s latest move to reduce the earnings of migrant workers will not only hurt migrants but it will drive down the wages of Kiwi workers. ...5 days ago
- Release: Nightmare before Christmas for Nicola Willis
With more debt and a larger deficit, Nicola Willis’ reputation is in tatters after her failure to return the Government’s books to surplus. ...5 days ago
- Warning to Fast-Track Applicants – ‘Exploit the Whenua, Face the Consequences’
Te Pāti Māori has this morning issued a stern warning to Fast-Track applicants with interests in mining, pledging to hold them accountable through retrospective liability and to immediately revoke Fast-Track consents under a future Te Pāti Māori government. This warning comes ahead of today’s third reading of the Fast-Track Approvals ...5 days ago
- Release: Govt cuts wages for lowest paid NZers… again
For the second year running, the government has effectively cut wages for the lowest paid workers in New Zealand. ...6 days ago
- Govt’s miserly 1.5% minimum wage will take workers backwards
The Government’s announcement today of a 1.5 per cent increase to minimum wage is another blow for workers, with inflation projected to exceed the increase, meaning it’s a real terms pay reduction for many. ...6 days ago
- Release: Govt shirking responsibility for rate hikes
All the Government has achieved from its announcement today is to continue to push responsibility back on councils for its own lack of action to help bring down skyrocketing rates. ...6 days ago
- Luxon’s ‘localism’ strikes again
The Government has used its final post-Cabinet press conference of the year to punch down on local government without offering any credible solutions to the issues our councils are facing. ...6 days ago
- Release: Govt breaks promise on EV chargers
The Government has failed to keep its promise to ‘super charge’ the EV network, delivering just 292 chargers - less than half of the 670 chargers needed to meet its target. ...6 days ago
- Greens call for end to subsidies for Methanex
The Green Party is calling for the Government to stop subsidising the largest user of the country’s gas supplies, Methanex, following a report highlighting the multi-national’s disproportionate influence on energy prices in Aotearoa. ...6 days ago
- Govt child poverty targets allow for increase in poverty
The Green Party is appalled with the Government’s new child poverty targets that are based on a new ‘persistent poverty’ measure that could be met even with an increase in child poverty. ...1 week ago
- Release: Four weeks annual leave under threat
The Government’s attack on workers continues with news it is scrapping work on the Holidays Act. ...1 week ago
- Govt’s emissions plan for measly 1% reduction
New independent analysis has revealed that the Government’s Emissions Reduction Plan (ERP) will reduce emissions by a measly 1 per cent by 2030, failing to set us up for the future and meeting upcoming targets. ...1 week ago
- Greens stand in solidarity with Whakaata Māori on sad day
The loss of 27 kaimahi at Whakaata Māori and the end of its daily news bulletin is a sad day for Māori media and another step backwards for Te Tiriti o Waitangi justice. ...1 week ago
- Sanctions regime to create more hardship for families
Yesterday the Government passed cruel legislation through first reading to establish a new beneficiary sanction regime that will ultimately mean more households cannot afford the basic essentials. ...1 week ago
- Govt gifts renters housing anxiety for Christmas
Today's passing of the Government's Residential Tenancies Amendment Bill–which allows landlords to end tenancies with no reason–ignores the voice of the people and leaves renters in limbo ahead of the festive season. ...1 week ago
- Release: National Party urged to support modern slavery legislation
Labour is urging the Prime Minister to walk the talk and support legislation combating modern slavery. ...2 weeks ago
- Release: Labour has lost confidence in the Speaker
The Speaker of the New Zealand Parliament made an unprecedented decision on the government amendment to the Fast Track Approvals Bill last night. ...2 weeks ago
- One year on, still no progress on new ferries
Today’s announcement from the Government on its plan for new ferries throws more uncertainty on the future of the country’s rail network. ...2 weeks ago
- Release: Nicola Willis’ smaller ferries will cost more
After wasting a year, Nicola Willis has delivered a worse deal for the Cook Strait ferries that will end up being more expensive and take longer to arrive. ...2 weeks ago
- Bill to sanction unlawful occupation of Palestine
Green Party co-leader Chlöe Swarbrick has today launched a Member’s Bill to sanction Israel for its unlawful presence in the Occupied Palestinian Territory, as the All Out For Gaza rally reaches Parliament. ...2 weeks ago
- Release: Labour fully supports greyhound racing ban
The Government has done the right thing in moving to ban greyhound racing. ...2 weeks ago
- Greyhound racing industry ban marks new era for animal welfare
After years of advocacy, the Green Party is very happy to hear the Government has listened to our collective voices and announced the closure of the greyhound racing industry, by 1 August 2026. ...2 weeks ago
- Rangatahi voices must be centred in Government’s Relationship and Sexuality Education refresh
In response to a new report from ERO, the Government has acknowledged the urgent need for consistency across the curriculum for Relationship and Sexuality Education (RSE) in schools. ...2 weeks ago
- Govt introduces archaic anti-worker legislation
The Green Party is appalled at the Government introducing legislation that will make it easier to penalise workers fighting for better pay and conditions. ...2 weeks ago
- Winston Peters – Kinleith Mill Speech
 Thank you for the invitation to speak with you tonight on behalf of the political party I belong to - which is New Zealand First. As we have heard before this evening the Kinleith Mill is proposing to reduce operations by focusing on pulp and discontinuing “lossmaking paper production”. They say that they are currently consulting on the plan to permanently shut ...2 weeks ago
Thank you for the invitation to speak with you tonight on behalf of the political party I belong to - which is New Zealand First. As we have heard before this evening the Kinleith Mill is proposing to reduce operations by focusing on pulp and discontinuing “lossmaking paper production”. They say that they are currently consulting on the plan to permanently shut ...2 weeks ago - Swarbrick calls on Auckland Mayor to end delay of revival of St James Theatre
Auckland Central MP, Chlöe Swarbrick, has written to Mayor Wayne Brown requesting he stop the unnecessary delays on St James Theatre’s restoration. ...2 weeks ago
- He Ara Anamata: Greens launch Emissions Reduction Plan
Today, the Green Party of Aotearoa proudly unveils its new Emissions Reduction Plan–He Ara Anamata–a blueprint reimagining our collective future. ...2 weeks ago
- Internationally-trained doctors jump at chance to boost health workforce
 Health Minister Dr Shane Reti says Health New Zealand will move swiftly to support dozens of internationally-trained doctors already in New Zealand on their journey to employment here, after a tripling of sought-after examination places. “The Medical Council has delivered great news for hardworking overseas doctors who want to contribute ...13 hours ago
Health Minister Dr Shane Reti says Health New Zealand will move swiftly to support dozens of internationally-trained doctors already in New Zealand on their journey to employment here, after a tripling of sought-after examination places. “The Medical Council has delivered great news for hardworking overseas doctors who want to contribute ...13 hours ago - PM appoints business leader to APEC Business Advisory Council
Prime Minister Christopher Luxon has appointed Sarah Ottrey to the APEC Business Advisory Council (ABAC). “At my first APEC Summit in Lima, I experienced firsthand the role that ABAC plays in guaranteeing political leaders hear the voice of business,” Mr Luxon says. “New Zealand’s ABAC representatives are very well respected and ...2 days ago
- New intelligence oversight appointments
Prime Minister Christopher Luxon has announced four appointments to New Zealand’s intelligence oversight functions. The Honourable Robert Dobson KC has been appointed Chief Commissioner of Intelligence Warrants, and the Honourable Brendan Brown KC has been appointed as a Commissioner of Intelligence Warrants. The appointments of Hon Robert Dobson and Hon ...2 days ago
- New housing developments able to progress more quickly
Improvements in the average time it takes to process survey and title applications means housing developments can progress more quickly, Minister for Land Information Chris Penk says. “The government is resolutely focused on improving the building and construction pipeline,” Mr Penk says. “Applications to issue titles and subdivide land are ...2 days ago
- Actions to speed up air travel delivering results
The Government’s measures to reduce airport wait times, and better transparency around flight disruptions is delivering encouraging early results for passengers ahead of the busy summer period, Transport Minister Simeon Brown says. “Improving the efficiency of air travel is a priority for the Government to give passengers a smoother, more reliable ...2 days ago
- Ending contracted emergency housing in Rotorua
The Government today announced the intended closure of the Apollo Hotel as Contracted Emergency Housing (CEH) in Rotorua, Associate Housing Minister Tama Potaka says. This follows a 30 per cent reduction in the number of households in CEH in Rotorua since National came into Government. “Our focus is on ending CEH in the Whakarewarewa area starting ...2 days ago
- Vocational education and training decisions support return to regions
The Government will reshape vocational education and training to return decision making to regions and enable greater industry input into work-based learning Tertiary Education and Skills Minister, Penny Simmonds says. “The redesigned system will better meet the needs of learners, industry, and the economy. It includes re-establishing regional polytechnics that ...2 days ago
- Reducing the environmental impact of synthetic refrigerants
The Government is taking action to better manage synthetic refrigerants and reduce emissions caused by greenhouse gases found in heating and cooling products, Environment Minister Penny Simmonds says. “Regulations will be drafted to support a product stewardship scheme for synthetic refrigerants, Ms. Simmonds says. “Synthetic refrigerants are found in a ...3 days ago
- Ngāruawāhia section of Waikato Expressway back to 4 lanes for Christmas
People travelling on State Highway 1 north of Hamilton will be relieved that remedial works and safety improvements on the Ngāruawāhia section of the Waikato Expressway were finished today, with all lanes now open to traffic, Transport Minister Simeon Brown says.“I would like to acknowledge the patience of road users ...3 days ago
- Appointments to the ENZ board
Tertiary Education and Skills Minister, Penny Simmonds, has announced a new appointment to the board of Education New Zealand (ENZ). Dr Erik Lithander has been appointed as a new member of the ENZ board for a three-year term until 30 January 2028. “I would like to welcome Dr Erik Lithander to the ...3 days ago
- Government to celebrate Waitangi Day around NZ
The Government will have senior representatives at Waitangi Day events around the country, including at the Waitangi Treaty Grounds, but next year Prime Minister Christopher Luxon has chosen to take part in celebrations elsewhere. “It has always been my intention to celebrate Waitangi Day around the country with different ...3 days ago
- More gangs added to Gangs Act list
Two more criminal gangs will be subject to the raft of laws passed by the Coalition Government that give Police more powers to disrupt gang activity, and the intimidation they impose in our communities, Police Minister Mark Mitchell says. Following an Order passed by Cabinet, from 3 February 2025 the ...3 days ago
- Judicial appointment announced
Attorney-General Judith Collins today announced the appointment of Justice Christian Whata as a Judge of the Court of Appeal. Justice Whata’s appointment as a Judge of the Court of Appeal will take effect on 1 August 2025 and fill a vacancy created by the retirement of Hon Justice David Goddard on ...3 days ago
- GDP data highlights importance of growth
The latest economic figures highlight the importance of the steps the Government has taken to restore respect for taxpayers’ money and drive economic growth, Finance Minister Nicola Willis says. Data released today by Stats NZ shows Gross Domestic Product fell 1 per cent in the September quarter. “Treasury and most ...3 days ago
- Strengthening Free Speech in Universities
Tertiary Education and Skills Minister Penny Simmonds and Associate Minister of Education David Seymour today announced legislation changes to strengthen freedom of speech obligations on universities. “Freedom of speech is fundamental to the concept of academic freedom and there is concern that universities seem to be taking a more risk-averse ...3 days ago
- Launch of Emergency Cellular Priority Service
Police Minister, Mark Mitchell, and Internal Affairs Minister, Brooke van Velden, today launched a further Public Safety Network cellular service that alongside last year’s Cellular Roaming roll-out, puts globally-leading cellular communications capability into the hands of our emergency responders. The Public Safety Network’s new Cellular Priority service means Police, Wellington ...3 days ago
- Minister reopens Mangamuka Gorge
State Highway 1 through the Mangamuka Gorge has officially reopened today, providing a critical link for Northlanders and offering much-needed relief ahead of the busy summer period, Transport Minister Simeon Brown says.“The Mangamuka Gorge is a vital route for Northland, carrying around 1,300 vehicles per day and connecting the Far ...4 days ago
- Funding confirmed for second Ashburton Bridge
The Government has welcomed decisions by the NZ Transport Agency (NZTA) and Ashburton District Council confirming funding to boost resilience in the Canterbury region, with construction on a second Ashburton Bridge expected to begin in 2026, Transport Minister Simeon Brown says. “Delivering a second Ashburton Bridge to improve resilience and ...4 days ago
- Government boosts support for avian influenza response
The Government is backing the response into high pathogenic avian influenza (HPAI) in Otago, Biosecurity Minister Andrew Hoggard says. “Cabinet has approved new funding of $20 million to enable MPI to meet unbudgeted ongoing expenses associated with the H7N6 response including rigorous scientific testing of samples at the enhanced PC3 ...4 days ago
- Levelling the playing field for media advertising
Legislation that will repeal all advertising restrictions for broadcasters on Sundays and public holidays has passed through first reading in Parliament today, Media Minister Paul Goldsmith says. “As a growing share of audiences get their news and entertainment from streaming services, these restrictions have become increasingly redundant. New Zealand on ...4 days ago
- Inspector-General of Defence appointed
Today the House agreed to Brendan Horsley being appointed Inspector-General of Defence, Justice Minister Paul Goldsmith says. “Mr Horsley’s experience will be invaluable in overseeing the establishment of the new office and its support networks. “He is currently Inspector-General of Intelligence and Security, having held that role since June 2020. ...4 days ago
- Fire and Emergency New Zealand final levy rates confirmed
Minister of Internal Affairs Brooke van Velden says the Government has agreed to the final regulations for the levy on insurance contracts that will fund Fire and Emergency New Zealand from July 2026. “Earlier this year the Government agreed to a 2.2 percent increase to the rate of levy. Fire ...4 days ago
- More AML relief on the way for Kiwi businesses
The Government is delivering regulatory relief for New Zealand businesses through changes to the Anti-Money Laundering and Countering Financing of Terrorism Act. “The Anti-Money Laundering and Countering Financing of Terrorism Amendment Bill, which was introduced today, is the second Bill – the other being the Statutes Amendment Bill - that ...4 days ago
- Hawke’s Bay Expressway moving at pace
Transport Minister Simeon Brown has welcomed further progress on the Hawke’s Bay Expressway Road of National Significance (RoNS), with the NZ Transport Agency (NZTA) Board approving funding for the detailed design of Stage 1, paving the way for main works construction to begin in late 2025.“The Government is moving at ...4 days ago
- Government seeks partnerships to plant trees on Crown-owned-land
The Government today released a request for information (RFI) to seeking interest in partnerships to plant trees on Crown-owned land with low farming and conservation value (excluding National Parks) Forestry Minister Todd McClay announced. “Planting trees on Crown-owned land will drive economic growth by creating more forestry jobs in our regions, providing more wood ...4 days ago
- Wide ranging legislation to make justice system more efficient
Court timeliness, access to justice, and improving the quality of existing regulation are the focus of a series of law changes introduced to Parliament today by Associate Minister of Justice Nicole McKee. The three Bills in the Regulatory Systems (Justice) Amendment Bill package each improve a different part of the ...4 days ago
- Diverse skills in community trust appointments
A total of 41 appointments and reappointments have been made to the 12 community trusts around New Zealand that serve their regions, Associate Finance Minister Shane Jones says. “These trusts, and the communities they serve from the Far North to the deep south, will benefit from the rich experience, knowledge, ...4 days ago
- Torture redress for survivors of the Lake Alice Unit
The Government has confirmed how it will provide redress to survivors who were tortured at the Lake Alice Psychiatric Hospital Child and Adolescent Unit (the Lake Alice Unit). “The Royal Commission of Inquiry into Abuse in Care found that many of the 362 children who went through the Lake Alice Unit between 1972 and ...4 days ago
- A busy year in the House
It has been a busy, productive year in the House as the coalition Government works hard to get New Zealand back on track, Leader of the House Chris Bishop says. “This Government promised to rebuild the economy, restore law and order and reduce the cost of living. Our record this ...4 days ago
- Consultation opens on working with engineered stone
“Accelerated silicosis is an emerging occupational disease caused by unsafe work such as engineered stone benchtops. I am running a standalone consultation on engineered stone to understand what the industry is currently doing to manage the risks, and whether further regulatory intervention is needed,” says Workplace Relations and Safety Minister ...5 days ago
- Greater reporting on Treaty settlement commitments
Mehemea he pai mō te tangata, mahia – if it’s good for the people, get on with it. Enhanced reporting on the public sector’s delivery of Treaty settlement commitments will help improve outcomes for Māori and all New Zealanders, Māori Crown Relations Minister Tama Potaka says. Compiled together for the ...5 days ago
- New appointments to the Charities Registration Board
Mr Roger Holmes Miller and Ms Tarita Hutchinson have been appointed to the Charities Registration Board, Community and Voluntary Sector Minister Louise Upston says. “I would like to welcome the new members joining the Charities Registration Board. “The appointment of Ms Hutchinson and Mr Miller will strengthen the Board’s capacity ...5 days ago
- Building consent processing times improve
More building consent and code compliance applications are being processed within the statutory timeframe since the Government required councils to submit quarterly data, Building and Construction Minister Chris Penk says. “In the midst of a housing shortage we need to look at every step of the build process for efficiencies ...5 days ago
- Faster access to support through Innovation Fund
Mental Health Minister Matt Doocey is proud to announce the first three recipients of the Government’s $10 million Mental Health and Addiction Community Sector Innovation Fund which will enable more Kiwis faster access to mental health and addiction support. “This fund is part of the Government’s commitment to investing in ...5 days ago
- New Zealand to assist Vanuatu on earthquake response
New Zealand is providing Vanuatu assistance following yesterday's devastating earthquake, Foreign Minister Winston Peters says. "Vanuatu is a member of our Pacific family and we are supporting it in this time of acute need," Mr Peters says. "Our thoughts are with the people of Vanuatu, and we will be ...5 days ago
- Government takes steps to reduce card fees for Kiwis
The Government welcomes the Commerce Commission’s plan to reduce card fees for Kiwis by an estimated $260 million a year, Commerce and Consumer Affairs Minister Andrew Bayly says.“The Government is relentlessly focused on reducing the cost of living, so Kiwis can keep more of their hard-earned income and live a ...5 days ago
- Review recommends ECE regulation shakeup
Regulation Minister David Seymour has welcomed the Early Childhood Education (ECE) regulatory review report, the first major report from the Ministry for Regulation. The report makes 15 recommendations to modernise and simplify regulations across ECE so services can get on with what they do best – providing safe, high-quality care ...5 days ago
- Offshore Renewable Energy Bill passes first reading
The Government‘s Offshore Renewable Energy Bill to create a new regulatory regime that will enable firms to construct offshore wind generation has passed its first reading in Parliament, Energy Minister Simeon Brown says.“New Zealand currently does not have a regulatory regime for offshore renewable energy as the previous government failed ...5 days ago
- Local Government (Water Services) Bill passes first reading
Legislation to enable new water service delivery models that will drive critical investment in infrastructure has passed its first reading in Parliament, marking a significant step towards the delivery of Local Water Done Well, Local Government Minister Simeon Brown and Commerce and Consumer Affairs Minister Andrew Bayly say.“Councils and voters ...5 days ago
- Gene Technology Bill passes first reading
New Zealand is one step closer to reaping the benefits of gene technology with the passing of the first reading of the Gene Technology Bill, Science, Innovation and Technology Minister Judith Collins says. "This legislation will end New Zealand's near 30-year ban on gene technology outside the lab and is ...5 days ago
- Signs of the hīkoi: More than just ‘words on cardboard’
 The placards seen at the Hīkoi mō Te Tiriti conveyed "huge kōrero with immediacy", expert says: "People know the power of the word." ...9 hours ago
The placards seen at the Hīkoi mō Te Tiriti conveyed "huge kōrero with immediacy", expert says: "People know the power of the word." ...9 hours ago - A final Ode to .. King Luxon
 Cosmic CatastropheThe year draws to a close.King Luxon has grown tired of the long eveningsListening to the dreary squabbling of his Triumvirate.He strolls up to the top floor of the PalaceTo consult with his Astronomer Royal.The Royal Telescope scans the skies,And King Luxon stares up into the heavensFrom the terrestrial ...17 hours ago
Cosmic CatastropheThe year draws to a close.King Luxon has grown tired of the long eveningsListening to the dreary squabbling of his Triumvirate.He strolls up to the top floor of the PalaceTo consult with his Astronomer Royal.The Royal Telescope scans the skies,And King Luxon stares up into the heavensFrom the terrestrial ...17 hours ago - A hater and an enthusiast review The Royal Free by Carl Shuker
 Spinoff editor Mad Chapman and books editor Claire Mabey debate Carl Shuker’s new novel about… an editor. Claire: Hello Mad, you just finished The Royal Free – overall impressions? Mad: Hi Claire, I literally just put the book down and I would have to say my immediate impression is ...18 hours ago
Spinoff editor Mad Chapman and books editor Claire Mabey debate Carl Shuker’s new novel about… an editor. Claire: Hello Mad, you just finished The Royal Free – overall impressions? Mad: Hi Claire, I literally just put the book down and I would have to say my immediate impression is ...18 hours ago - Survive to 25 (December, that is)
Christmas and its buildup are often lonely, hard and full of unreasonable expectations. Here’s how to make it to Jesus’s birthday and find the little bit of joy we all deserve. Have you found this year relentless? Has the latest Apple update “fucked up your life”? Have you lost two ...18 hours ago
- All I want for Christmas is modern day slavery legislation
Despite overwhelming public and corporate support, the government has stalled progress on a modern day slavery law. That puts us behind other countries – and makes Christmas a time of tragedy rather than joy, argues Shanti Mathias. Picture the scene on Christmas Day. Everyone replete with nice things to eat, ...18 hours ago
- Israeli-American historian describes attacks on Gaza as ‘war of annihilation’
 Asia Pacific Report “It looks like Hiroshima. It looks like Germany at the end of World War Two,” says an Israeli-American historian and professor of holocaust and genocide studies at Brown University about the horrifying reality of Gaza. Professor Omer Bartov, has described Israel’s ongoing war on Gaza as an ...21 hours ago
Asia Pacific Report “It looks like Hiroshima. It looks like Germany at the end of World War Two,” says an Israeli-American historian and professor of holocaust and genocide studies at Brown University about the horrifying reality of Gaza. Professor Omer Bartov, has described Israel’s ongoing war on Gaza as an ...21 hours ago - NZ govt plans to make ‘heavy handed’ change to free speech rules for universities
The New Zealand government coalition is tweaking university regulations to curb what it says is an increasingly “risk-averse approach” to free speech. The proposed changes will set clear expectations on how universities should approach freedom of speech issues. Each university will then have to adopt a “freedom of speech statement” ...21 hours ago
- Caitlin Johnstone: Where does the aggression really begin?
Report by Dr David Robie – Café Pacific. – COMMENTARY: By Caitlin Johnstone New York prosecutors have charged Luigi Mangione with “murder as an act of terrorism” in his alleged shooting of health insurance CEO Brian Thompson earlier this month. This news comes out at the same time as ...1 day ago
- OECD Report Highlights That More Is Needed
 This report reflects that gap in our dealings overseas, and it shows that legislators, the public sector and businesses need to walk the talk. ...1 day ago
This report reflects that gap in our dealings overseas, and it shows that legislators, the public sector and businesses need to walk the talk. ...1 day ago - Government quietly scraps waste minimisation policies
The government has quietly cancelled plans to improve recycling and roll out a kerbside food scraps composting scheme. ...1 day ago
- MEAA welcomes News MAP funding ‘leg up’ for Australian journalism
Pacific Media Watch The union for Australian journalists has welcomed the delivery by the federal government of more than $150 million to support the sustainability of public interest journalism over the next four years. Combined with the announcement of the revamped News Bargaining Initiative, this could result in up to ...1 day ago
- Transmission Gully partnership breakdown will not hurt future public-private partnerships, Infrastru...
The roads partnership unravelled under a confidential settlement this week, meaning NZTA will now finish off what it had said was incomplete work. ...2 days ago
- Funding cuts to charity particularly felt over Christmas period
The number of people seeking help from Lifeline is expected to increase by 10 to 20 percent over Christmas. ...2 days ago
- Nelson Hospital conditions ‘unbearable’ – staff
One worker says the building is decrepit and falling down around them. ...2 days ago
- The Secret Diary of .. Luxon at Xmas
MONDAY“Merry Xmas, and praise the Lord,” said Sheriff Luxon, and smiled for the camera. There was a flash of smoke when the shutter pressed down on the magnesium powder. The sheriff had arranged for a photographer from the Dodge Gazette to attend a ceremony where he handed out food parcels to ...2 days ago
- Stand by for cricket’s Smash Palace
It’s a little under two months since the White Ferns shocked the cricketing world, deservedly taking home the T20 World Cup. Since then the trophy has had a tour around the country, five of the squad have played in the WBBL in Australia while most others have returned to domestic ...2 days ago
- Early-onset dementia under the microscope
Comment: If we say the word ‘dementia’, many will picture an older person struggling to remember the names of their loved ones, maybe a grandparent living out their final years in an aged care facility. Dementia can also occur in people younger than 65, but it can take time before ...2 days ago
- Keeping the pirates at bay: Should the Australian ‘Blocking Order’ case prompt a discussion in N...
Piracy is a reality of modern life – but copyright law has struggled to play catch-up for as long as the entertainment industry has existed. As far back as 1988, the House of Lords criticised copyright law’s conflict with the reality of human behaviour in the context of burning cassette ...2 days ago
- ‘We were as famous as Tom Cruise’: Craig Parker on 90s Shortland St fandom
As he makes a surprise return to Shortland Street, actor Craig Parker takes us through his life in television. Craig Parker has been a fixture on television in Aotearoa for nearly four decades. He had starring roles in iconic local series like Gloss, Mercy Peak and Diplomatic Immunity, featured in ...2 days ago
- ‘I prioritise the mission, not my health’: Adam McGrath’s perfect weekend playlist
The Ōtautahi musician shares the 10 tracks he loves to spin, including the folk classic that cured him of a ‘case of the give-ups’. When singer-songwriter Adam McGrath returns to Kumeu’s Auckland Folk Festival from January 24-27, he’s not planning on simply idling his way through – he wants the late ...2 days ago
- The rescue dog bringing joy to Christchurch retirement homes
Alex Casey spends an afternoon on the job with River, the rescue dog on a mission to spread joy to Ōtautahi rest homes. Almost everyone says it is never enough time. But River the rescue dog, a jet black huntaway border collie cross, has to keep a tight pace to ...2 days ago
- Fiji pro-Palestine nativity scene exposes Gaza as ‘hell on earth’ at Christmas
Asia Pacific Report Fiji activists have recreated the nativity scene at a solidarity for Palestine gathering in Fiji’s capital Suva just days before Christmas. The Fiji Women’s Crisis Centre and Fijians for Palestine Solidarity Network recreated the scene at the FWCC compound — a baby Jesus figurine lies amidst the ...2 days ago
- Vanuatu quake: ‘Our shop was flattened like a deck of cards’
By 1News Pacific correspondent Barbara Dreaver and 1News reporters A number of Kiwis have been successfully evacuated from Vanuatu after a devastating earthquake shook the Pacific island nation earlier this week. The death toll was still unclear, though at least 14 people were killed according to an earlier statement from ...2 days ago
- How diplomats have broken the law in NZ – and what happened next
A handful of foreign diplomats have misbehaved during their time here - and not all of them have been brought to justice. ...2 days ago
- Swim schools report sinking enrolments as downturn deepens
Being able to swim is often considered a life skill, but tough economic times are forcing many families to pull their children out of lessons. ...2 days ago
- ‘There will be deaths because of this’ – Warning over Health NZ IT cuts
A West Coast IT worker is warning patients will die as Health New Zealand aims to slash its data and digital staff. ...2 days ago
- Polytech sales possible but unlikely when Te Pūkenga disestablished – minister
In a surprise move, the sale of polytechnics will be on the table when the national institute of technology Te Pūkenga is disestablished. ...2 days ago
- Parliament’s final sitting day an insight into party factions
On Parliament's last day of the year, there was a rare glimpse of the factions within the major parties. ...2 days ago
- Former Labour MP, North Shore mayor Ann Hartley dies
Former Labour MP and mayor of Auckland's North Shore City Ann Hartley has died. ...2 days ago
- The closest thing Australian cartooning had to a prophet: the sometimes celebrated, sometimes contro...
Source: The Conversation (Au and NZ) – By Richard Scully, Professor in Modern History, University of New England Bunker. Image courtesy of Michael Leunig, CC BY-NC-SA Michael Leunig – who died in the early hours of Thursday December 19, surrounded by “his children, loved ones, and sunflowers” – was the ...2 days ago
- Labour moves Speaker from the ‘nice’ to ‘naughty’ list
Last week's fights with the Speaker over the Fast Track schedule may have changed the tone in Parliament. ...2 days ago
- Govt ends pilot programme for Māori and Pacific, sparking outrage
The Government announced the end of the programme that allowed Māori and Pacific people to acess bowel cancer screening at 50-years-old. ...2 days ago
- Parliament fits an extra morning into final sitting day
The House - On Parliament's last day of the year, there was the rare occurrence of a personal (conscience) vote on selling booze over the Easter weekend. While it didn't have the numbers to pass, it was a chance to get a rare glimpse of the fact ...2 days ago
- The Friday Poem: ‘Bejeweled log’ by Holly Fletcher
A new poem by Holly Fletcher. bejeweled log i was dreaming about wasps / wee darlings that followed me / ducking under objects / that i was fated to pickup / my fingers seeking / and meeting with tiny proboscis’s / but instead / i wake up / roll sideways ...2 days ago
- Sunglasses don’t just look good – they’re good for you too. Here’s how to choose the right p...
Source: The Conversation (Au and NZ) – By Flora Hui, Research Fellow, Centre for Eye Research Australia and Honorary Fellow, Department of Surgery (Ophthalmology), The University of Melbourne Versta/Shutterstock Australians are exposed to some of the highest levels of solar ultraviolet (UV) radiation in the world. While we ...2 days ago
- How does franchising work?
Source: The Conversation (Au and NZ) – By Andrew Terry, Professor of Business Regulation, University of Sydney Michael von Aichberger/Shutterstock Even if you’ve no idea how the business model underpinning franchises works, there’s a good chance you’ve spent money at one. Franchising is essentially a strategy for cloning ...2 days ago
- The one episode of Shortland Street you need to watch this year
If something big is going to happen in Ferndale, it’s going to happen at Christmas. This is an excerpt from our weekly pop culture newsletter Rec Room. Sign up here. If there’s one episode of Shortland Street you should watch each year, it’s the annual Christmas cliffhanger. The final episode of ...2 days ago
- As China expands its cyber espionage and sabotage operations, how will the Trump administration resp...
Source: The Conversation (Au and NZ) – By William A. Stoltz, Lecturer and expert Associate, National Security College, Australian National University US President-elect Donald Trump has named most of the members of his proposed cabinet. However, he’s yet to reveal key appointees to America’s powerful cyber warfare and intelligence institutions. ...2 days ago
- The Unity Books bestseller chart for 2024
Announcing the top 10 books of the the year at Unity Books’ stores in High St, Auckland, and Willis St, Wellington. AUCKLAND 1 Intermezzo by Sally Rooney (Faber & Faber, $37) The phenomenal Irish writer is the unsurprising chart topper for 2024 with her fourth novel that, much like her first ...2 days ago
- Government confirms plan to dismantle Te Pūkenga, re-establish polytechs
The government has confirmed its plan to break up Te Pūkenga / New Zealand Institute of Skills and Technology and re-establish independent polytechnics. ...2 days ago
Thank you LPent.
I'm a bit older than you, Lynn. I remember queuing up at primary school for a polio vaccine (oral) and BCG test for TB. the TB test involved being kind of stamped with multiple skin pricks in one shot, on the wrist.
I recall being scared when I heard an adult down our street was partially paralysed as a result of polio. Eventually I confided my fear in my mother at bedtime. She reassured me I wouldn't get it, cos she and Dad hadn't got it, etc.
The first couple of times I travelled overseas, I had cholera injections, and small pox scratch-type vaccines on my shoulder – still have the scar. Whilst travelling the cholera shots had to be renewed about every 6 months, and recorded on my vaccination card.
Disease outbreaks were pretty common in the UK and Ireland in the 19th century (open sewers were a cause) – worst was during the potato famine in Ireland when typhus was rife there.
Typhoid also was one of the factors that ended the dominance of classical Athens – due to unhealthy sanitation – throwing slops and sewage out windows, etc.
These are the reasons why we have our current sewage and rubbish collection systems.
I imagine the 21st century viruses will result in preventive systems being developed, domestically, and in relation to overseas travel. Our border control systems will change long term. And probably we will end for good, hand shaking, travelling about town when sick, packing people like sardines into mass transport services, etc.
As a result of my experiences in my younger days, I take preventive measures seriously.
We didn't stop any of that after Sars, Mers and other sars virus that we don't hear of that were not so viable, and like all those with a bit of luck this Sars virus will die out too. It is mainly because it needs a host to remain viable and can only remain viable for hours or days at the most outside the human body. The problem will be if it can remain viable long term in those who are immune to it but so far that does not seem to be happening. It spread in Wuhan because it was given time to be hosted by thousands and spread worldwide within that time.
That is why all the talk is about breaking the chain. We are lucky here that this brilliantly led Government is taking the best advice possible and treating it with the respect it deserves unlike most of the incompetent right-wing dickheads in the rest of the world.
I am thinking of preventive measures to prevent further outbreaks of new viruses. I understand places like Sth Korea already had systems and resources in place after the initial SARS outbreak, focused on responding quickly to any new viruses that may arise. So they were able to respond quickly to Covid-19.
Exactly Carolyn, I don't think we thought this one would get this far but I'm pretty sure a certain level of preparedness is/was in place. The difference for this mongrels spread is that it is "silent "for up to five days or longer while being diffused through the community, which the experts don't think had been happened before in Sars like pathogens.
I'd like to think that the answer to it may lie in why others can seem to fight it off sometimes without even knowing it. I bet researchers are looking there already.
As I pointed out in that long post, that is part of the problem. From the viruses 'perspective' having the host running their immune system ‘hot’ or even dying on it while it is breeding is a bad bet.
From my reading on covid-19, the thing that causes most of the nasty symptoms and death appears to be your own immune systems trying to deal too strongly with an intruder too late. That is what gives you the really bad cough and sneeze reflexes to clear viruses out of the lungs. It is what causes the lung inflammation which appears to be the usual cause of death.
The elderly have on average more sluggish immune systems. They react much slower to bugs and viruses. Moreover their immune systems frequently overreact especially with lung inflammation.
Younger people without compromised immune systems are faster reacting to catch the invading virus and triggering the second tier of immune responses (ie past the initial layer of fever, coughing, and sneezing) earlier and preventing a build up of virus load.
Problem is that while some people may only be mildly symptomatic, they’re still trailing a trail of generated viruses for many days after their symptoms die down. Unfortunately that really just means that they’re more productive at breeding the virus because they will usually wind up infecting more unsuspecting people they come into contact with.
Imagine if Joyce and his cronies were still in charge? Or Bridges for that matter. Even when it's clear Australia, US and the UK have missed the boat we're still being told this sort of shit. Hopefully, when this is all over, the lunacy of the right will become apparent to the general population:
https://www.stuff.co.nz/national/politics/opinion/120649991/how-will-we-exit-the-lockdown
I don’t think you can dismiss what Steven Joyce has written as shit. The economic cost of this shutdown will be massive, and as usual those on lower incomes will be hardest hit. It will be almost as important as the timing of the start of the shutdown as when we decide to finish it, or scale it back.
These things do need to be considered fairly soon to have some sort of plan trying to get back to normal.
Sure, the timing of the end of the shutdown will be important, but Joyce is suggesting starting to open things up at the end of the four weeks unless it's clear things aren't improving – a slightly watered down version of what Trump's been saying up until his recent change of tone.
The innumerate Stephen Joyce?
No fan of Joyce but the article seems reasonably reasonable.
Pretty legal, you think?
I'm the same age as Lynn, by the way, but had much the same experiences as you.
My mother had polio during the epidemic. She was one of the fortunate ones. They both tell me how scary it was hearing about classmates dying.
Actually, on further thought I think I had the test and oral vaccination at secondary school – maybe 3rd form. So those of you a bit younger may have had them at primary school.
I think our parents went through some tough times in the 1920s-50s.
Staying a home, physical distancing, loss of income still probably very tolerable for many of us. As always, it is those on low incomes and with underlying health issues that we need to support. Let's hope the majority of the country step up to do that.
What seems to be lacking at the moment is any evidence of human immunity developing to covid-19. Without immunity we will continue to be hit again and again, and isolation efforts will only delay the inevitable.
Death is inevitable for all – in a Covid-19 context, delay has much to recommend it.
The fact that people are recovering means their immune systems are working and developing immunity.
What is unclear is how long that immunity lasts, and/or how quickly the virus evolves to the point of being able to re-infect someone that had previously developed immunity.
While it is indeed possible that we'll have to deal with repeating waves of equal (or worse) severity, what is far more likely is that some degree of immunity will develop and future waves will be less severe. It's also reasonably likely that with enough time vaccines and/or pharmaceutical therapies will be developed. Then the usual evolution trajectory for infectious diseases is to become less harmful – it's really not beneficial for an organism to kill its host.
This virus, like all coronaviruses, mutates and over time, it might become less harmful. In practice, this could mean that it will travel around the globe causing seasonal spikes in disease and deaths, just like ordinary flu.
Depends on the rate that covid-19 'mutates' (actually mostly how often it incorporates other species rna).
Influenza is a promiscuous as hell. So far the SARS-COV-x viruses don't appear to be.
Long may that continue…
https://www.stuff.co.nz/national/health/coronavirus/120656955/eight-strains-of-the-coronavirus-are-circling-the-globe-theyre-giving-scientists-clues
A nice read, even for a non-science audience.
yeah it was a good article and a good site NextStrain.org
Try hitting the play button on… https://nextstrain.org/ncov
A charming tale.
https://nymag.com/intelligencer/2020/03/the-story-of-a-coronavirus-infection.html
https://en.wikipedia.org/wiki/Jeff_Wise
From an historical perepective have a read of Pepys Diary during the plague years, 1665/1666
http://www.pepys.info/1665/plague.html
"I, for one, have absolutely no real interest in dying for tourism."
I think you're not alone in that sentiment. Even family members who work in the tourist industry are questioning its future viability/validity.
An interesting point raised in the book Justinian's Flea is the relationship of the rise of the plague, and a extended period of warmer temperatures. We are set for a very extended period of warmer temperatures, I don't like our prospects.
I also don't like our prospects of keeping isolation down here at the bottom of the south seas. We lack some basic industries to be isolated. My hope is out of this, we start building some self–sustaining industry here for ourselves.
I agree with DV Iprent, and thank you. It has clarified a lot of issues for a thick clod like myself.
Because of the lower numbers now entering the country why are they not all being tested. Are we ( the Government) that dim.
I can't speak for the government's reasoning, but for my reckons:
Detecting community transmission and stopping it is a big factor in determining when we can drop alert levels. We have limited testing resources, so it seems to make most sense to use it for detecting cases that transmitted within New Zealand, rather than wasting the resource on known risks that can be managed other ways.
Starting March 15 everyone coming in had been required to self-isolate for two weeks, prior to the four-week lockdown we now have. At the moment, that precaution appears more than adequate to ensure they won't spread any disease they had on arrival.
Andre I accept the importance of community testing but surely stopping them coming in is paramount. On the AM show this morning there was talk of a private company in NZ capable of supplying test kits and has been trying to get the Government to take some interest for two weeks. Without any luck to date. We all know some people just don’t self isolate don’t we Andre. We know the Government has its protocols but maybe they should look outside of their bubble.
This private company, are they the ones in joe90's first comment in today's Open Mike? https://thestandard.org.nz/open-mike-30-03-2020/#comment-1696221
Also, when it comes to arseholes that repay the privilege of being allowed back in the midst of a pandemic by breaking self-isolation, there's other ways of dealing with them. Personally I'm not averse to the idea of just shooting them, but I accept I'm probably out on the fringes of public opinion on that one. There’s still no need to further privilege them by wasting limited testing resources on all of them for the sake of finding the very few that are both infected and antisocial enough to break self-isolation.
What would be the purpose of testing them? Returning citizens either have a satisfactory self-isolation plan or are carted off to a dedicated quarantine hotel for two weeks, so if they have the virus that will be revealed by the isolation period. It therefore makes no sense to waste much-needed test kits on those people rather than putting them to good use pinning down community transmission.
Sorry PM but those who are supposedly self isolating would think twice about breaking ranks if a phone call came through with a positive. Just because you and I say we’re going to do this properly doesn’t mean everybody will. It’s my point of view and I can’t see why it’s a wasted test where you would also have their contact number and be able to reinforce the message if a positive turns up rather than trying to chase them up after the fact when they didn’t self isolate properly and put the community at risk.
New View – you seem to think the test is infallible. As I understand, during the early stage of infection, the test shows negative, It is not infallible. Isolation and time is a more valid test – the isolation just has to be enforced.
You are correct. For all tests, there is a trade-off between sensitivity and specificity.
https://en.wikipedia.org/wiki/Sensitivity_and_specificity
No I don’t think the test is infallible’ I think it’s a big red light for those who might get a positive to be on super alert with their isolation. Those not displaying symptoms but positive might be tempted to push the isolation boundaries to the detriment of the community. If there is only a few hundred coming into the country on a daily basis wouldn’t you just test to be on the safe side and close one more door. Silly me for being overly careful.
Silly you. The isolation has to be enforced, and that is the only fail-proof test. Test kits which we are short of are needed more elsewhere. Obviously.
No 'safe side' at all as you conjecture.
As you will know it can’t be enforced in every case. I hope for our sakes it is enforced but can’t be. I personally know of returned friends that have isolated but only by chance. I won’t describe their complete circumstances but will say only that they live in a rural area and it was only their immediate family that reinforced the isolation. Other families may not be so lucky. The private company shown on the AM show could have supplied quick kits to the Government but they weren’t interested. Would have been fine for airport use even though slightly less accurate. I guess the Government knows best. 😔 🤪
Yes, they do and they made the right decision IMHO.
Yes it’s just your opinion as I have mine. You don’t explain why you think the Government have got this decision right.
Because it is a different type of test than the standard PCR-based one.
But don’t take my word for it, as you don’t know me, take the word of Dr Siouxsie Wiles: https://thespinoff.co.nz/science/31-03-2020/covid-19-what-difference-can-the-new-fast-turnaround-blood-tests-make/
I think that GPs are now testing, or getting tested, the people they think most likely to be Covid-19 positive. They need to be selective because the labs don't have the resources to test everyone. Testing of a sample of the general population should indicate the extent of community transmission, and likely hot spots.
When I had a phone consultation with a GP last Monday, I got that impression. I have a scratchy throat – more likely strep throat than the virus. She prescribed antibiotics.
I said I had been doing social/physical distancing as much as possible for the last few weeks, and hadn't had close contact with anyone in that period.
The GP said to self-isolate & stay away from other people just in case it's Covid-19. She said she wasn't going to get me tested for the virus – I don't have a fever or runny nose and feel fine. Also she said I'm a healthy 70 yr old without any underlying condition.
I haven't been out of my flat since then, except to put out rubbish & check the mailbox.
Aren't facts amazing – I don't why we bother with fiction:
Virus Wars – MRC LMB www2.mrc-lmb.cam.ac.uk › viruswars › viruses
www2.mrc-lmb.cam.ac.uk › viruswars › viruses
Every day you breathe in over 100,000,000 viruses. … Each antibody producing cell can produce 2000 antibody molecules per second. … by our white blood cells and are a major part of the body's response to combatting a viral infection.
For those who want all the nitty-gritty, in academic-speak (and it has coloured pics which make it easier to comprehend).
https://onlinelibrary.wiley.com/doi/10.1002/jmv.25685 Journal of Medical Virology (Free Access!)
Coronavirus infections and immune responses
(It includes quite a list a list of receptors – I think we should bring the Welcome doormat inside, myself. Then it goes on to Type 1 interferons, dendritic cells and defensins. This is the perfect link to swot up on so you can bat everyone else's mere opinions, with, seemingly, perfect authority!)
Evolution is relentless. The more one species exploits its environment the more other species will respond, die or exploit.
The fastest are microbial, fungi etc.
CVD19 just struck it lucky in evolutionary Lotto
The space humans have been taking over the planet is obviously unsustainable.
As we become extinct Ther are plenty of organisms available to exploit what is left.
WE ARE IN THIS ALL TOGETHER, (regardless of what boris trump and/or donald johnson have to say about it.
Evolution will out.
My grandmother walked with a brace her whole life because of polio. I got a shot.
i got rubella (german measles), I was kept away from school for a month, because everyone in NZ knew someone who knew someone who had had a child who had a birth defect because their mother had contracted it during pregnancy. Mothers kept us home because it could have been them, or us.
My kids got chicken pox literally the week before the vaccine became available – they might have shingles when they are old (but there is a vaccine).
The only reason we have anti-vaxxers is because we have forgotten all this – these are family stories we need to tell our kids, grandkids, etc so that no one forgets
I, for one, have absolutely no real interest in dying for tourism
We have had avalanche after avalanche of Tourism in recent years, the Faeces from which has been strewn freely the length and breadth of the country.
Somebody must have made $millions. But why were they allowed to bring huge overloads of visitors ?
When the Governments of the past 40 years should have been building State houses ! By now, the words "LandLord" and "Homeless" should have vanished from Aotearoa.
It would be nice if Kiwis who live here get to see their own Nation. At realistic Cost.